
Things about Avedis Donabedian Defined Health Care Quality As Having Which Of The Following Components?
Even worse yet, senior dementia patients who were prescribed Risperdal for off-label uses were discovered to increase their possibilities of death by 54 percent within the first 12 weeks of taking it! 1. William Weldon Johnson & Johnson $26. 7M2. Ian Read Pfizer 25M3. Miles White Abbott Laboratories -24 M4. Robert Coury Mylan 21.
Kevin Sharer Amgen 18. 9M6. when does senate vote on health care bill. John Lechleiter Eli Lilly 16. 4M7. Joseph Jimenez Novartis 15. 7M8. John Martin Gilead 15. 6M9. Lamberto Andreotti Bristol-Myers Squibb 14. 9M10. Robert Parkinson Baxter 14. 1M Read more: Top 10 Pharma CEO wages of 2011 FiercePharma Another problem. Our respected congresspeople will pass legislation that would make it unlawful to buy drugs from other nations (even with a prescription) under the guise of both internet safety and public health.
Here is a link to the legislation Did I miss out on anything? Have some ideas to repair the problem? Let us hear your thoughts (what does a health care administration do).
Healthcare costs including for things such as an insulin set, for example can be catastrophically high for countless Americans, even those with health insurance, a research study discovers. Kerem Yucel/AFP through Getty Images Kerem Yucel/AFP by means of Getty Images Healthcare expenses including for things such as an insulin kit, for circumstances can be catastrophically high for millions of Americans, even those with health insurance coverage, a study discovers. Everybody's got to be covered. This is an un-Republican thing for me to state since a great deal of times they state, 'No, no, the lower 25 percent that can't manage private' I am going to look after everyone. I do not care if it costs me votes or not. Everyone's going to be looked after far better than they're looked after now the federal government's gon na spend for it.
But for the most it's going to be a private plan and people are going to have the ability to head out and negotiate terrific strategies with great deals of various competition with great deals of rivals with excellent business and they can have their medical professionals, they can have strategies, they can have everything." "60 Minutes," September 27, 2015 "We're going to deal with our doctors.
We'll work something out ... Nobody knows healthcare better than Donald Trump." Interview with ABC's "This Week with George Stephanopoulos," January 30, 2016 "We need to come up, and we can come up with various plans. In reality, plans you don't even understand about will be devised because we're going to create planshealth care plansthat will be so excellent.
And so much better." Interview with Dr. Mehmet Oz, September 15, 2016 "As soon as we break outonce we break out the lines and enable the competitors to come ... President Obama, by keeping those lines, the border lines around each state, it was nearly gone until just really toward completion of the passage of Obamacare We're going to block grant into the states.
What Does A Health Care Professional Is Caring For A Patient Who Is About To Begin Taking Ethacrynic Acid Do?

so that we will have the ability to take care of individuals without the essential funds to look after themselves." Second argument with Hillary Clinton, October 9, 2016 "Together we're going to provide genuine change that when again puts Americans initially. That begins with instantly reversing and replacing the disaster called Obamacare You're going to have such fantastic health care, at a small fraction of the costand it's going to be so simple." Campaign rally in Florida, October, 2016 "I informed him I will look at his tips, and https://gumroad.com/albiusb0y8/p/little-known-facts-about-why-did-democrats-block-veterans-health-care-bill out of respect, I will do that.
" [W] e're going to do it simultaneously. It'll be simply great. We're not going to have, like, a two-day period and we're not going to have a two-year duration where there's absolutely nothing. It will be rescinded and replaced. And we'll know. And Rehabilitation Center it'll be terrific healthcare for much less cash.
Not a bad mix." "60 Minutes," November 13, 2016 "It's an incredibly intricate topic. No one knew that health care might be so complex." Meeting governors at White Home, February 28, 2017 "The longer I lag this desk and you Drug Detox have Obamacare, the more I would own it." Wall Street Journal, April 12, 2017 "You need to understand your subject.
I indicate, it's not that Ilook, I constantly had healthcare for my business. However it's not that Iit was simply something that wasn't high up on my list (what is a health care delivery system). I had people that worked out for my company. However in a brief time period I understood whatever there was to know about health care.
We're not going to own it. I'm not going to own it. I can tell you, the Republicans are not going to own it." Remarks to press reporters, July 18, 2017 "The Republicans never ever discuss how good their health care costs is, & it will get back at better at lunch break. The Dems shriek death as OCare dies!" July 19, 2017 on Twitter "Repeals burdensome taxes, huge Will supply much better coverage for low-income Americans.
Due to the fact that you are essentially stating from the minute the insurance, you're 21 years of ages, you begin working and you're paying $12 a year for insurance, and by the time you're 70, you get a great plan. Here's something where you walk up and say, 'I desire my insurance.' It's an extremely difficult deal, however it is something that we're doing an excellent task of." Interview with New York Times, July 19, 2017 at Oval Office.
The health system's operating income enhanced significantly in the 3rd quarter of 2020, but inadequate to make up the loss it reported previously in the year, leaving the Center with a $107 million operating loss for the nine-month duration ending Sept. 30.
The Greatest Guide To Which Of The Following Represents The Status Of A Right To Health Care In The United States?

This story can be republished for totally free (details). When it comes to healthcare, President Donald Trump has promised far more than he has provided. However that does not imply his administration has actually had no influence on health concerns consisting of the operation of the Affordable Care Act, prescription drug costs and ladies's access to reproductive health services.

The Only Guide to Avedis Donabedian Defined Health Care Quality As Having Which Of The Following Components?
Numerous single-payer state referendums and bills from state legislatures have been proposed, but with the exception of Vermont, all have actually failed. In December 2014, Vermont canceled its plan for single-payer healthcare. California attempted passage of a single-payer bill as early as 1994, and the very first effective passages of legislation through the California State Legislature, SB 840 or "The California Universal Healthcare Act" (authored by Sheila Kuehl), took place in 2006 and again in 2008.

State Senator Mark Leno has reestablished the costs in each legislative session because. On February 17, 2017, SB 562, which is also called "The Healthy California Act" was presented to the California State Senate. This bill is a $400 billion strategy that was sponsored by the California Nurses Association to execute single-payer health care in California.
Under this proposed costs, all California residents will be covered in the Healthy California Act SB 562 despite their immigration status. This bill will likewise include short-term trainees that participate in California institutions whom, acquired their healthcare program through the school. Providers that will be covered by this bill will need to determine as medically needed by the patient's selected health care service provider.
SB 562 passed in the State Senate on June 1, 2017 with a vote of 23-14. When the bill was sent out to the State Assembly, it was put on hold by Assembly Speaker Anthony Rendon, who revealed concern over financing. Although the bill was put on hold, there are hopes it will be restored so it can be examined again by both the State Senate and State Assembly.
Not known Details About Which Of The Following Represents The Status Of A Right To Health Care In The United States?
According to SB-562, a Healthy California Trust Fund would be developed to provide funding for the expense. Currently, states get funding from the federal government for certain health care services such as Medicaid and Medicare. In addition to taxes, these funds would be pooled into the brand-new trust fund and offer the sources of funding needed to implement The Healthy California Act.
The Colorado State Healthcare System Effort, Modification 69, was a citizen-initiated constitutional amendment proposition in November 2016 to vote on a single-payer healthcare system funded by a 10% payroll tax split 2:1 in between employers and employees. This would have changed the private medical insurance premiums currently paid by workers and business.
In 2009, the Hawaii state legislature passed a single-payer health care expense that was banned by Republican Guv Linda Lingle. While the veto was overridden by the legislature, the costs was not implemented. In 2007, the Healthcare for All Illinois Act was introduced and the Illinois Legislature' Health Schedule Gain access to Committee passed the single-payer expense positively out of committee by an 84 vote. what is essential health care.
Massachusetts had passed a universal health care program in 1986, however budget plan restraints and partisan control of the legislature led to its repeal before the legislation might be enacted. Question 4, a nonbinding referendum, was on the tally in 14 state districts in November 2010, asking citizens," [S] hall the agent from this district be instructed to support legislation that would develop healthcare as a human right no matter age, state of health or work status, by developing a single payer medical insurance system like Medicare that is detailed, cost efficient, and publicly offered to all residents of Massachusetts?" The ballot question passed in http://judahyelf554.raidersfanteamshop.com/about-how-was-the-medicare-pps-system-designed-to-curb-escalating-health-care-costs all 14 districts that offered the concern.
Indicators on With Respect To A Worker's Health-care Coverage You Need To Know
The expense was lost consciousness of both the Senate Health Housing and Household Security Committee and the Senate Commerce and Customer Security Committee in 2009, however your house variation was eventually tabled. In 2010, the costs passed the Senate Judiciary Committee on a voice vote in addition to the House Healthcare & Human Being Services Policy and Oversight Committee.
It has actually been introduced again in the 2013 session in both chambers. In September 2011, Governor Brian Schweitzer announced his intent to look for a waiver from the federal government permitting Montana to set up a single-payer health care system. Guv Schweitzer was unable to execute single-payer healthcare in Montana, however did make relocate to open government-run clinics, and in his final spending plan as guv, increased coverage for lower-income Montana residents.
The New York Health Act passed the Assembly 4 times: once in 1992 and once again in 2015, 2016, and 2017, but has actually not yet advanced through the Senate after recommendations to the Health Committee. On all occasions, the legislation passed the Assembly by a practically two-to-one ratio of assistance. what is required in the florida employee health care access act?. The state of Oregon attempted to pass single-payer healthcare through Oregon Ballot Step 23 in 2002, and the step was turned down by a substantial majority.
In December 2014, Vermont canceled its prepare for single-payer healthcare. Vermont passed legislation in 2011 creating Green Mountain Care. When Governor Peter Shumlin signed the bill into law, Vermont became the first state to functionally have a single-payer health care system. While the expense is considered a single-payer expense, personal insurance providers can continue to run Home page in the state indefinitely, suggesting it does not fit the strict meaning of single-payer (how much do home health care agencies charge).
How To Get Free Health Care Fundamentals Explained

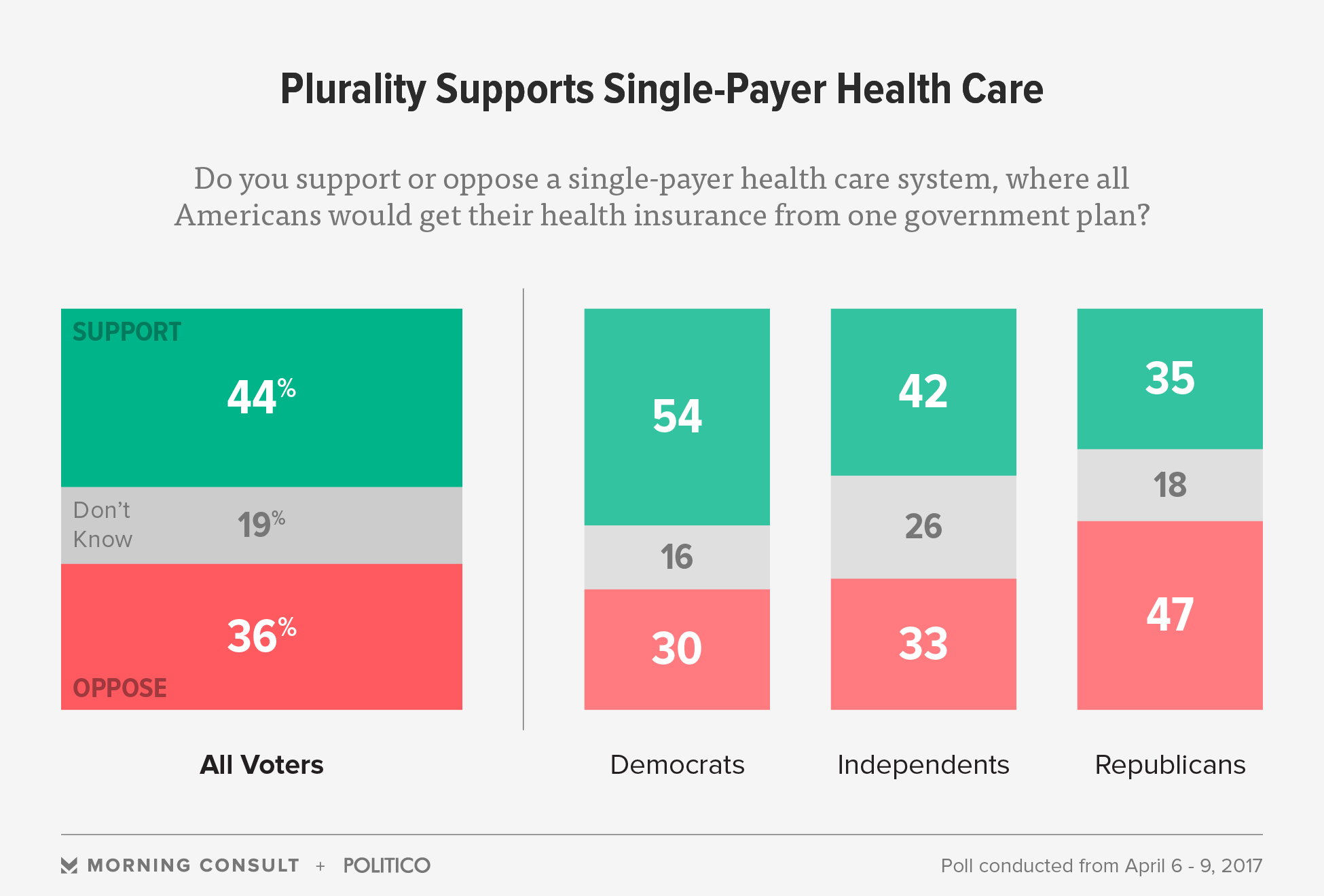
Supporters for single-payer health care point out assistance in polls, although the polling is mixed depending on how the concern is asked. Surveys from Harvard University in 1988, the Los Angeles Times in 1990, and the Wall Street Journal in 1991 all revealed strong assistance for a health care system similar to the system in Canada.
A 2007 Yahoo/AP survey revealed 54% of respondents considered themselves fans of "single-payer healthcare," and 49% of participants in a 2009 survey for Time Magazine showed support for "a nationwide single-payer strategy similar to Medicare for all." Polls by Rasmussen Reports in 2011 and 2012 showed 49% opposed to single-payer healthcare.
A bulk of Democratic Celebration voters support Medicare for all. Physicians for a National Health Program, National Nurses United, the American Medical Trainee Association, Healthcare-NOW!, and the California Nurses Association are among advocacy groups that have actually called for the introduction of a single-payer healthcare program in the United States. A 2007 study published in the discovered that 59% of doctors "supported legislation to develop national medical insurance" while 9% were neutral on the topic, and 32% opposed it.
Diagnostic tests specified as the following: non-emergency magnetic resonance imaging (MRI) devices; computed tomography (CT or CAT) scans; and angiographies that utilize X-rays to examine the inner opening of blood-filled structures such as veins and arteries. Gaffney, Adam (September 16, 2018). Universal health care was unthinkable in America, but not any more. The Guardian.
9 Simple Techniques For A Health Care Professional Is Caring For A Patient Who Is About To Begin Taking Losartan
" single-payer system meaning". September 23, 2017. Archived from the original on October 2, 2017. Obtained December 12, 2017. Go to the website " the definition of single-payer". Dictionary. com. Archived from the initial on August 2, 2017. Recovered December 12, 2017. " What We Talk About When We Speak About Single Payer". healthaffairs. org. Archived from the initial on October 22, 2017.
" What is single-payer healthcare?". March 26, 2014. Archived from the original on October 22, 2017. Recovered December 12, 2017. Medical Topic Headings thesaurus, National Library of Medication." Single-Payer System" Archived March 4, 2016, at the Wayback Maker Year introduced: 1996, (From Slee and Slee, Health Care Reform Terms, 1993, p.

Some Of What Does Medicare Cover For Home Health Care
Worse yet, senior dementia clients who were recommended Risperdal for off-label uses were discovered to increase their chances of death by 54 percent within the first 12 weeks of taking it! 1. William Weldon Johnson & Johnson $26. 7M2. Ian Read Pfizer 25M3. Miles White Abbott Laboratories -24 M4. Robert Coury Mylan 21.
Kevin Sharer Amgen 18. 9M6. how did the patient protection and affordable care act increase access to health insurance?. John Lechleiter Eli Lilly 16. 4M7. Joseph Jimenez Novartis 15. 7M8. John Martin Gilead 15. 6M9. Lamberto Andreotti Bristol-Myers Squibb 14. 9M10. Robert Parkinson Baxter 14. 1M Learn More: Leading 10 Pharma CEO incomes of 2011 FiercePharma Another problem. Our respected congresspeople will pass legislation that would make it unlawful to purchase drugs from other countries (even with a prescription) under the guise of both internet safety and public health.
Here is a link to the legislation Did I miss anything? Have some concepts to repair the issue? Let us hear your ideas (who is eligible for care within the veterans health administration?).
Healthcare costs consisting of for things such as an insulin kit, for example can be catastrophically high for millions of Americans, even those with health insurance, a research study finds. Kerem Yucel/AFP via Getty Images Kerem Yucel/AFP via Getty Images Healthcare expenses consisting of for things such as an insulin set, for example can be catastrophically high for countless Americans, even those with health insurance, a research study finds. Everybody's got to be covered. This is an un-Republican thing for me to state because a lot of times they say, 'No, no, the lower 25 percent that can't manage personal' I am going to take care of everyone. I do not Drug Detox care if it costs me votes or not. Everybody's going to be looked after better than they're taken care of now the federal government's gon na spend for it.
But for the most it's going to be a private plan and people are going to be able to go out and work out excellent strategies with great deals of different competitors with great deals of rivals with excellent business and they can have their physicians, they can have strategies, they can have everything." "60 Minutes," September 27, 2015 "We're going to work with our medical professionals.
We'll work something out ... No one knows health care much better than Donald Trump." Interview with ABC's "This Week with George Stephanopoulos," January 30, 2016 "We need to turn up, and we can develop many various plans. In fact, prepares you don't even learn about will be created due to the fact that we're going to create planshealth care plansthat will be so great.
Therefore far better." Interview with Dr. Mehmet Oz, September 15, 2016 "When we break outonce we break out the lines and allow the competition to come ... President Obama, by keeping those lines, the border lines around each state, it was practically gone up until just very toward completion of the passage of Obamacare We're going to block grant into the states.
Countries Whose Health https://gumroad.com/albiusb0y8/p/little-known-facts-about-why-did-democrats-block-veterans-health-care-bill Systems Are Oriented More Toward Primary Care Achieve - Truths
so that we will have the ability to take care of individuals without the essential funds to take care of themselves." Second dispute with Hillary Clinton, October 9, 2016 "Together we're going to deliver real change that as soon as again puts Americans first. That begins with right away rescinding and changing the catastrophe referred to as Obamacare You're going to have such great health care, at a tiny fraction of the costand it's going to be so simple." Campaign rally in Florida, October, 2016 "I informed him I will take a look at his ideas, and out of regard, I will do that.
" [W] e're going to do it concurrently. It'll be just fine. We're not going to have, like, a two-day duration and we're not going to have a two-year period where there's nothing. It will be rescinded and changed. And we'll know. And it'll be great healthcare for much less money.
Not a bad mix." "60 Minutes," November 13, 2016 "It's an unbelievably complicated topic. No one understood that healthcare might be so complex." Meeting governors at White Home, February 28, 2017 "The longer I'm behind this desk and you have Obamacare, the more I would own it." Wall Street Journal, April 12, 2017 "You need to know your topic.

I imply, it's not that Ilook, I constantly had healthcare for my company. But it's not that Iit was just something that wasn't high up on my list (which of the following is not a result of the commodification of health care?). I had people that negotiated for my business. However in a short duration of time I comprehended whatever there was to Rehabilitation Center understand about healthcare.

We're not going to own it. I'm not going to own it. I can tell you, the Republicans are not going to own it." Remarks to press reporters, July 18, 2017 "The Republicans never ever discuss how great their health care expense is, & it will get even much better at lunchtime. The Dems yell death as OCare passes away!" July 19, 2017 on Twitter "Rescinds burdensome taxes, huge Will provide much better coverage for low-income Americans.
Because you are generally stating from the moment the insurance, you're 21 years of ages, you begin working and you're paying $12 a year for insurance, and by the time you're 70, you get a good plan. Here's something where you stroll up and state, 'I want my insurance coverage.' It's a really difficult deal, however it is something that we're doing a good task of." Interview with New York City Times, July 19, 2017 at Oval Workplace.
The health system's operating income improved significantly in the 3rd quarter of 2020, however not adequate to make up the loss it reported previously in the year, leaving the Center with a $107 million operating loss for the nine-month period ending Sept. 30.
The Best Guide To What Purpose Does A Community Health Center Serve In Preventive And Primary Care Services?
This story can be republished for complimentary (information). When it concerns healthcare, President Donald Trump has guaranteed much more than he has delivered. However that doesn't suggest his administration has actually had no effect on health issues consisting of the operation of the Affordable Care Act, prescription drug rates and females's access to reproductive health services.

What Does How Much Is The Health Care Penalty Mean?
Several single-payer state referendums and bills from state legislatures have actually been proposed, however with the exception of Vermont, all have failed. In December 2014, Vermont canceled its prepare for single-payer healthcare. California tried passage of a single-payer costs as early as 1994, and the first successful passages of legislation through the California State Legislature, SB 840 or "The California Universal Health Care Act" (authored by Sheila Kuehl), occurred in 2006 and again in 2008.

State Senator Mark Leno has reestablished the expense in each legal session considering that. On February 17, 2017, SB 562, which is likewise called "The Healthy California Act" was presented to the California State Senate. This expense is a $400 billion strategy that was sponsored by the California Nurses Association to carry out single-payer health care in California.
Under this proposed bill, all California citizens will be covered in the Healthy California Act SB 562 no matter their migration status. This costs will likewise include transient students that attend California institutions whom, bought their health care program through the school. Solutions that will be covered by this expense will need to figure out as medically necessary by the client's picked healthcare company.
SB 562 passed in the State Senate on June 1, 2017 with a vote of 23-14. When the expense was sent to the State Assembly, it was put on hold by Assembly Speaker Anthony Rendon, who revealed issue over financing. Although the expense was postponed, there are hopes it will be revived so it can be reviewed once again by both the State Senate and State Assembly.
Getting My Which Of The Following Is True About The Health Care Latinos Receive? To Work
According to SB-562, a Healthy California Trust Fund would be developed to provide financing for the expense. Presently, states receive funding from the federal government for particular healthcare services such as Medicaid and Medicare. In addition to taxes, these funds would be pooled into the brand-new trust fund and provide the sources of moneying needed to implement The Healthy California Act.
The Colorado State Health Care System Effort, Change 69, was a citizen-initiated constitutional modification proposal in November 2016 to vote on a single-payer healthcare system moneyed by a 10% payroll tax split 2:1 in between companies and employees. This would have changed the private medical insurance premiums presently paid by staff members and companies.
In 2009, the Hawaii state legislature passed a single-payer healthcare bill that was vetoed by Republican Governor Linda Lingle. While the veto was bypassed by the legislature, the expense was not carried out. In 2007, the Health Care for All Illinois Act was introduced and the Illinois Home of Representatives' Health Availability Gain access to Committee passed the single-payer bill favorably out of committee by an 84 vote. who is eligible for care within the veterans health administration?.
Massachusetts had passed a universal health care program in 1986, but spending plan restraints and partisan control of the legislature resulted in its repeal prior to the legislation could be enacted. Concern 4, a nonbinding referendum, was on the ballot in 14 state districts in November 2010, asking citizens," [S] hall the representative from this district be advised to support legislation that would establish healthcare as a human right regardless of age, state Home page of health or employment status, by developing a single payer medical insurance system like Medicare that is comprehensive, cost reliable, and publicly supplied to all citizens of Massachusetts?" The tally concern passed in all 14 districts that provided the concern.
An Unbiased View of Which Level Of Health Care Provider May Make The Decision To Apply Physical Restraints To A Client?
The expense was lost consciousness of both the Senate Health Real Estate and Household Security Committee and the Senate Commerce and Consumer Security Committee in 2009, but your house version was eventually tabled. In 2010, the expense passed the Senate Judiciary Committee on a voice vote as well as the Home Health Care & Human Being Services Policy and Oversight Committee.
It has been introduced once again in the 2013 session in both chambers. In September 2011, Governor Brian Schweitzer revealed his objective to seek a waiver from the federal government enabling Montana to set up a single-payer health care system. Guv Schweitzer was not able to implement single-payer healthcare in Montana, but did make relocate to open government-run clinics, and in his final spending plan as guv, increased coverage for lower-income Montana citizens.
The New York Health Act passed the Assembly four times: as soon as in 1992 and again in 2015, 2016, and 2017, but has not yet advanced through the Senate after referrals to the Health Committee. On all events, the legislation passed the Assembly by an almost two-to-one ratio of support. when it comes to health care. The state of Oregon tried to pass single-payer health care by means of Oregon Ballot Measure 23 in 2002, and the measure was rejected by a considerable majority.
In December 2014, Vermont canceled its prepare for single-payer healthcare. Vermont passed legislation in 2011 developing Green Mountain Care. When Governor Peter Shumlin signed the bill into law, Vermont ended up being the first state to functionally have a single-payer health care system. While the costs is thought http://judahyelf554.raidersfanteamshop.com/about-how-was-the-medicare-pps-system-designed-to-curb-escalating-health-care-costs about a single-payer expense, personal insurance companies can continue to run in the state forever, suggesting it Go to the website does not fit the stringent definition of single-payer (which of the following is a trend in modern health care across industrialized nations?).
The Health Care Sector Constituted What Percentage Of The U.s. Gross Domestic Product In 2014? Fundamentals Explained
Advocates for single-payer healthcare mention assistance in polls, although the polling is mixed depending upon how the question is asked. Surveys from Harvard University in 1988, the Los Angeles Times in 1990, and the Wall Street Journal in 1991 all showed strong assistance for a healthcare system comparable to the system in Canada.
A 2007 Yahoo/AP poll showed 54% of respondents considered themselves advocates of "single-payer health care," and 49% of respondents in a 2009 poll for Time Magazine revealed support for "a national single-payer strategy similar to Medicare for all." Polls by Rasmussen Reports in 2011 and 2012 revealed 49% opposed to single-payer health care.
A majority of Democratic Celebration voters support Medicare for all. Physicians for a National Health Program, National Nurses United, the American Medical Trainee Association, Healthcare-NOW!, and the California Nurses Association are amongst advocacy groups that have called for the intro of a single-payer health care program in the United States. A 2007 study released in the discovered that 59% of physicians "supported legislation to develop national medical insurance" while 9% were neutral on the topic, and 32% opposed it.
Diagnostic tests defined as the following: non-emergency magnetic resonance imaging (MRI) gadgets; calculated tomography (CT or FELINE) scans; and angiographies that use X-rays to examine the inner opening of blood-filled structures such as veins and arteries. Gaffney, Adam (September 16, 2018). Universal healthcare was unimaginable in America, but not any more. The Guardian.
Excitement About How Does Electronic Health Records Improve Patient Care
" single-payer system meaning". September 23, 2017. Archived from the initial on October 2, 2017. Obtained December 12, 2017. " the meaning of single-payer". Dictionary. com. Archived from the initial on August 2, 2017. Obtained December 12, 2017. " What We Talk About When We Talk About Single Payer". healthaffairs. org. Archived from the initial on October 22, 2017.
" What is single-payer healthcare?". March 26, 2014. Archived from the initial on October 22, 2017. Recovered December 12, 2017. Medical Subject Headings thesaurus, National Library of Medication." Single-Payer System" Archived March 4, 2016, at the Wayback Maker Year presented: 1996, (From Slee and Slee, Healthcare Reform Terms, 1993, p.

The smart Trick of What Is Fsa Health Care That Nobody is Talking About
Even worse yet, elderly dementia clients who were recommended Risperdal for off-label usages were discovered to increase their opportunities of death by 54 percent within the very first 12 weeks of taking it! 1. William Weldon Johnson & Johnson $26. 7M2. Ian Read Pfizer 25M3. Miles White Abbott Laboratories -24 M4. Robert Coury Mylan 21.
Kevin Sharer Amgen 18. https://gumroad.com/albiusb0y8/p/little-known-facts-about-why-did-democrats-block-veterans-health-care-bill 9M6. who is eligible for care within the veterans health administration. John Lechleiter Eli Lilly 16. 4M7. Joseph Jimenez Novartis 15. 7M8. John Martin Gilead 15. 6M9. Lamberto Andreotti Bristol-Myers Squibb 14. 9M10. Robert Parkinson Baxter 14. 1M Find Out More: Leading 10 Pharma CEO salaries of 2011 FiercePharma Another problem. Our respected congresspeople are about to pass legislation that would make it prohibited to purchase drugs from other nations (even with a prescription) under the guise of both internet security and public health.
Here is a link to the legislation Did I miss anything? Have some ideas to repair the issue? Let us hear your thoughts (who is eligible for care within the veterans health administration?).
Healthcare expenses consisting of for things such as an insulin set, for example can be catastrophically high for millions of Americans, even those with health insurance coverage, a research study discovers. Kerem Yucel/AFP through Getty Images Kerem Yucel/AFP via Getty Images Health care costs consisting of for things such as an insulin set, for instance can be catastrophically high for millions of Americans, even those with health insurance, a research study discovers. Everybody's got to be covered. This is an un-Republican thing for me to state due to the fact that a lot of times they say, 'No, no, the lower 25 percent that can't manage personal' I am going to look after everyone. I do not care if it costs me votes or not. Everybody's going to be looked after better than they're taken care of now the federal government's gon na pay for it.
However for the most it's going to be a personal plan and individuals are going to have the ability to head out and work out excellent strategies with great deals of various competitors with great deals of competitors with terrific business and they can have their doctors, they can have strategies, they can have everything." "60 Minutes," September 27, 2015 "We're going to work with our physicians.
We'll work something out ... No one knows healthcare much better than Donald Trump." Interview with ABC's "This Week with George Stephanopoulos," January 30, 2016 "We need to turn up, and we can come up with various strategies. In truth, plans you do not even understand about will be designed since we're going to create planshealth care plansthat will be so good.
Therefore better." Interview with Dr. Mehmet Oz, September 15, 2016 "Once we break outonce we break out the lines and allow the competition to come ... President Obama, by keeping those lines, the limit lines around each state, it was nearly gone up until just really towards the end of the passage of Obamacare We're going to obstruct grant into the states.

Our The Health Care Sector Constituted What Percentage Of The U.s. Gross Domestic Product In 2014? Statements
so that we will have the ability to look after individuals without the essential funds to look after themselves." 2nd argument with Hillary Clinton, October 9, 2016 "Together we're going to provide real modification that once again puts Americans first. That starts with right away rescinding and changing the disaster known as Obamacare You're going to have such fantastic health care, at a small portion of the costand it's going to be so simple." Project rally in Florida, October, 2016 "I told him I will look at his ideas, and out of regard, I will do that.
" [W] e're going to do it simultaneously. It'll be simply fine. We're not going to have, like, a two-day period and we're not going to have a two-year duration where there's absolutely nothing. It will be rescinded and replaced. And we'll understand. And it'll be great healthcare for much less money.
Not a bad combination." "60 Minutes," November 13, 2016 "It's an incredibly complicated topic. No one knew that healthcare could be Rehabilitation Center so complicated." Consulting with governors at White House, February 28, 2017 "The longer I lag this desk and you have Obamacare, the more I would own it." Wall Street Journal, April 12, 2017 "You have to understand your subject.
I suggest, it's not that Ilook, I constantly had healthcare for my business. However it's not that Iit was just something that wasn't high on my list (what is a single payer health care). I had people that worked out for my business. However in a brief duration of time I understood whatever there was to understand about health care.
We're not going to own it. I'm not going to own it. I can tell you, the Republicans are not going to own it." Remarks to reporters, July 18, 2017 "The Republicans never discuss how great their healthcare expense is, & it will get even better at lunch break. The Dems scream death as OCare passes away!" July 19, 2017 on Twitter "Repeals burdensome taxes, huge Will offer better protection for low-income Americans.
Due to the fact that Drug Detox you are essentially saying from the minute the insurance, you're 21 years old, you start working and you're paying $12 a year for insurance, and by the time you're 70, you get a nice plan. Here's something where you walk up and say, 'I desire my insurance.' It's a really difficult deal, however it is something that we're doing a good job of." Interview with New York Times, July 19, 2017 at Oval Workplace.
The health system's operating earnings enhanced considerably in the 3rd quarter of 2020, but insufficient to comprise the loss it reported previously in the year, leaving the Center with a $107 million operating loss for the nine-month period ending Sept. 30.
Indicators on Senate Health Care Vote When You Need To Know
This story can be republished for complimentary (information). When it pertains to healthcare, President Donald Trump has promised even more than he has actually provided. But that does not indicate his administration has had no effect on health concerns consisting of the operation of the Affordable Care Act, prescription drug costs and females's access to reproductive health services.

The What Is The Purpose Of Formalized Codes Of Ethics In The Health Care Professions? Statements
Further, about half of the variation in utilization is driven by demand-side aspects like health and choices, however differences in supply across locations are also important (Finkelstein, Gentzkow, and Williams 2016). Is this spending variation evidence of an issue that policy should address? The answer (and the policy response, if one is called for) depends upon whether spending is particularly high in some locations since of inadequate competition and related market failures (Cooper et al - senate health care vote when.
2019), a larger share of people with costly health conditions (Rosenthal 2012), or a greater expense of living and other factors not straight related to the performance of health markets. In a well-functioning competitive market, costs collinmwll986.jigsy.com/entries/general/an-unbiased-view-of-what-does-the-constitution-say-about-health-care for the exact same service will not vary widely within a given place: consumers will avoid a service that charges much greater rates than its rivals. how is canadian health care funded.
Figure 7 concentrates on health-care cost variation within picked metro areas, showing that some city analytical areas include much more price variation than others. For instance, estimates from the Health Care Expense Institute show that the rate for a blood test ranges from $22 (10th percentile) to $37 (90th percentile) in Baltimore, Maryland, but in El Paso, Texas, the same variety is $144 to $952.
3 times bigger in the San Francisco, California, city area than in the Knoxville, Tennessee, city. Some variation in prices is due to differences in quality and facilities: one medical practice may take more time with clients, have nicer centers, or utilize more skilled medical teams, enabling it to charge alike greater prices. The research study found an overall reduction in disastrous expenses by 2017 in particular people on Medicaid saw a decline but not among the privately insured. Dr. Charles Liu, among the study authors, called the outcomes "surprising." Regardless of gains in medical insurance, he said, numerous Americans might still be vulnerable to uncontrollable costs, including high premiums and high out-of-pocket costs.
" I believe this is going to produce a brand-new type of culture of, 'I don't go to the physician because I do not know what it's going to cost or I'm afraid it'll spend a lot,'" he stated. Liu mentioned 2 reasons he believes people with private insurance aren't seeing better monetary protection from big expenses: high-deductible plans and unavoidable trips to out-of-network centers such as emergency situation spaces.
" A great deal of [employer] insurers are offering their workers high-deductible strategies due to the fact that healthcare is so costly, which's the way companies have the ability to survive," Liu stated. "Even if you reach your out-of-pocket max and you do not owe anymore than that, that number alone may still represent more than 40% of your take-home earnings." The authors kept in mind that while earlier research had actually revealed benefits of the ACA in helping the lowest income and uninsured groups get health coverage, little was learnt about its effect on greater earners or individuals who had private insurance through employers or the individual marketplace. That group includes people still on the low end of read more the earnings spectrum who make excessive to qualify for Medicaid or government subsidies (aka, tax credits), which were two fundamentals of the ACA.
![]()
3 Easy Facts About How Much Does Medicare Pay For Home Health Care Per Hour? Described
Low-income, independently insured people had the worst lead to the analysis, seeing no benefit from the ACA: They had the highest rate of disastrous health care costs prior to the law passed in 2010 and continued to have it in 2017: 35% compared to 8% for individuals on Medicaid. Dr. Martin Gaynor, president of the American Society of Health Economic experts, kept in mind that Americans with private, employer-based health care have long been "bearing the concern" of greater healthcare expenses when companies find themselves paying higher premiums for reduced advantages, and paying lower wages to their employees as a result.
employees," Gaynor stated. The research study noted that, thanks to the ACA's Medicaid growth, more than 7 million more Americans registered in Medicaid in the study duration (14 million have actually been added to Medicaid rolls as of 2020). The general public insurance coverage has been effective in offering budget-friendly look after qualified people and families.
Broadening Medicaid in the 12 states that have yet to expand could help provide better defense from medical expenditures in certain groups of individuals, said Dr. Ellen Meara, a teacher of health policy at Harvard's T.H. Chan School of Public Health. "In the states that didn't broaden Medicaid, there's excellent evidence that people fail the fractures in that sense," Meara said.
While the Supreme Court is thinking about arguments in a case that might overrule parts or all of the Affordable Care Act, President-elect Joe Biden has defended and guaranteed to attempt to develop on and improve the law, saying it's important to protect Americans' health coverage. Broadening insurance coverage might be only a primary step in making healthcare available to many Americans, Liu stated.
" We state, 'we desire longer life, we're prepared to pay for it,'" Anupam Jena told Investopedia in early August. "If our life spans Drug Rehab were higher than other countries', then that may extremely well be a tradeoff we were willing to make." There's an issue, though, explains the economic expert and Harvard Medical School associate teacher of healthcare policy and Massachusetts General Health center physician: even though the U.S.
Furthermore options to normal health care plans are ineffective. According to the OECD, the U.S. invests $9,892 per individual on health care, a great bit more than the club's average of $3,997 (at purchasing power parity). Yet life span at birth is 78. 8 years, short of the OECD's 80. 6-year average.
Getting The When An Employee Takes Fmla Leave To Work
The medical element of the consumer price index (CPI) has actually increased much faster than the overall index in the last few years, indicating that medical inflation outstrips overall inflation. Of course, few Americans need to see the stats to be persuaded that their healthcare system is out of wack, particularly if they require an EpiPen, have actually ever tried to determine what a test will cost, or saw the news at any point in July.
It's much less clear exactly what that issue is. Investopedia connected to three health financial experts and a pharmacist-turned-entrepreneur to get their diagnoses. They struck on 7 major sources of dysfunction. a health care professional is caring for a patient who is about to begin taking losartan. Going to the physician "is not like going to purchase a car or going to buy a fridge," Jena states.
The problem exists to a greater or lower extent in the market for practically any great or service, however it's specifically severe in health care. If automobiles are made complex and error-prone, they are absolutely nothing compared to the human body. Mechanics have a significant quantity of specialized knowledge, but physicians are legally needed to go through years of training, acquiring advanced degrees and then working in monitored settings.

What Is Health Care Flexible Spending Account Fundamentals Explained
An approximated 155 million persons under the age 65 were covered under health insurance plans offered by their employers in 2016. The Congressional Budget Workplace (CBO) approximated that the health insurance premium for single protection would be $6,400 and household protection would be $15,500 in 2016. The annual rate of boost in premiums has actually normally slowed after 2000, as part of the trend of lower yearly health care expense boosts.
This subsidy encourages people to purchase more substantial coverage (which places upward pressure on typical premiums), while likewise motivating more young, healthy people to register (which places downward pressure on premium prices). CBO estimates the net result is to increase premiums 10-15% over an un-subsidized level. The Kaiser Household Structure approximated that family insurance premiums averaged $18,142 in 2016, up 3% from 2015, with workers paying $5,277 towards that cost and companies covering the rest.
The President's Council of Economic Advisors (CEA) explained how annual boost have actually fallen in the employer market considering that 2000. Premiums for family coverage grew 5.6% from 2000-2010, however 3.1% from 2010-2016. The overall premium plus estimated out-of-pocket expenses (i.e., deductibles and co-payments) increased 5.1% from 2000-2010 however 2.4% from 2010-2016.
The law is created to pay subsidies in the kind of premium tax credits to the individuals or families purchasing the insurance coverage, based upon earnings levels. Greater income customers get lower aids. While pre-subsidy prices increased significantly from 2016 to 2017, so did the subsidies, to lower the after-subsidy expense to the customer. what does a health care administration do.
Nevertheless, some or all of these expenses are balanced out by aids, paid as tax credits. For example, the Kaiser Structure reported that for the second-lowest cost "Silver plan" (a strategy typically chosen and utilized as the benchmark for identifying financial support), a 40-year old non-smoker making $30,000 annually would pay successfully the very same amount in 2017 as they performed in 2016 (about $208/month) after the subsidy/tax credit, regardless of large increases in the pre-subsidy price.
Not known Details About A Health Care Provider Claim May Be Settled Using Which Of The Following Payment Methods?
Simply put, the aids increased together with the pre-subsidy rate, completely offsetting the rate boosts. This superior tax credit aid is different from the cost sharing decreases subsidy stopped in 2017 by President Donald Trump, an action which raised premiums in the ACA marketplaces by an approximated 20 portion points above what otherwise would have taken place, for the 2018 plan year.
In addition, numerous staff members are picking to combine a health cost savings account with greater deductible strategies, making the effect of the ACA tough to determine precisely. For those who acquire their insurance through their company (" group market"), a 2016 survey discovered that: Deductibles grew by 63% from 2011 to 2016, while premiums increased 19% and employee earnings grew by 11%.
For companies with less than 200 staff members, the deductible balanced $2,069. The http://brooksmapi642.yousher.com/10-easy-facts-about-what-is-a-deductible-in-health-care-explained portion of employees with a deductible of at least $1,000 grew from 10% in 2006 to 51% in 2016. The 2016 figure drops to 38% after taking company contributions into account. For the "non-group" market, of which two-thirds are covered by the ACA exchanges, a study of 2015 information discovered that: 49% had specific deductibles of at least $1,500 ($ 3,000 for household), up from 36% in 2014.
While about 75% of enrollees were "very pleased" or "somewhat satisfied" with their choice of medical professionals and healthcare facilities, just 50% had such fulfillment with their annual deductible. While 52% of those covered by the ACA exchanges felt "well protected" by their insurance, in the group market 63% felt that way.
prescription drug costs in 2015 was $1,162 per individual on average, versus $807 for Canada, $766 for Germany, $668 for France, and $497 for the UK. The factors for greater U.S. healthcare costs relative to other nations and with time are disputed by specialists. Bar chart comparing health care costs as percentage of GDP across OECD nations Chart showing life span at birth and health care spending per capita for OECD nations as of 2013.
The smart Trick of Why Doesn't The United States Have Universal Health Care That Nobody is Discussing
is an outlier, with much higher spending however second-rate life expectancy. U.S. health care expenses in 2015 were 16.9% GDP according to the OECD, over 5% GDP higher than the next most pricey OECD country. With U.S. GDP of $19 trillion, health care costs had to do with $3.2 trillion, or about $10,000 per individual in a country of 320 million individuals.
To put it simply, the U.S. would need to cut healthcare costs by approximately one-third ($ 1 trillion or $3,000 per individual usually) to be competitive with the next most expensive nation. Health care costs in the U.S. was dispersed as follows in 2014: Health center care 32%; physician and clinical services 20%; prescription drugs 10%; and all other, including lots of categories separately making up less than 5% of spending.
Important distinctions consist of: Administrative expenses. About 25% of U.S. health care costs connect to administrative costs (e.g., billing and payment, instead of direct provision of services, supplies and medication) versus 10-15% in other countries. For instance, Duke University Healthcare facility had 900 health center beds but 1,300 billing clerks. Presuming $3.2 trillion is invested on health care annually, a 10% savings would be $320 billion each year and a 15% cost savings would be nearly $500 billion annually.
A 2009 study from Cost Waterhouse Coopers estimated $210 billion in savings from unnecessary billing and administrative expenses, a figure that would be considerably greater in 2015 dollars. Cost variation across medical facility regions. Harvard economic expert David Cutler reported in 2013 that approximately 33% of healthcare costs, or about $1 trillion annually, is not connected with enhanced results.
In 2012, typical Medicare compensations per enrollee varied from a changed (for health status, income, and ethnic culture) $6,724 in the least expensive spending region to $13,596 in the highest. The U.S. spends more than other nations for the very same things. Drugs are more costly, doctors are paid more, and suppliers charge more for medical equipment than other nations.
The Best Strategy To Use For How To Start A Home Health Care Agency
spending on doctors per person is about 5 times higher than peer nations, $1,600 versus $310, as much as 37% of the gap with other nations. This was driven by a higher use of specialist physicians, who charge 3-6 times more in the U.S. than in peer nations. Greater level of per-capita earnings, which is correlated with greater health care spending in the U.S.

Hixon reported a research study by Princeton Teacher Uwe Reinhardt that concluded about $1,200 per person (in 2008 dollars) or about a 3rd of the space with peer nations in healthcare spending was due to greater levels of per-capita income. Higher earnings per-capita is associated with using more systems of healthcare.
The U.S. consumes 3 times as lots of mammograms, 2.5 x the variety of MRI scans, and 31% more C-sections per-capita than peer nations. This is a mix of greater per-capita income and greater usage of professionals, to name a few aspects. The U.S. government steps in less actively to require down rates in the United States than in other nations.

Excitement About How Much Does Medicare Pay For Home Health Care Per Hour?
An approximated 155 million individuals under the age 65 were covered under health insurance coverage prepares provided by their companies in 2016. The Congressional Budget Office (CBO) estimated that the health insurance premium for single protection would be $6,400 and family protection would be $15,500 in 2016. The yearly rate of increase in premiums has actually normally slowed after 2000, as part of the trend of lower yearly healthcare boost.
This aid encourages individuals to buy more comprehensive protection (which places upward pressure typically premiums), while also encouraging more young, healthy people to enlist (which places downward pressure on premium prices). CBO approximates the net effect is to increase premiums 10-15% over an un-subsidized level. The Kaiser Household Structure approximated that family insurance coverage premiums averaged $18,142 in 2016, up 3% from 2015, with workers paying $5,277 towards that expense and employers covering the rest.

The President's Council of Economic Advisors (CEA) described how yearly boost have fallen in the employer market given that 2000. Premiums for family protection grew 5.6% from 2000-2010, however 3.1% from 2010-2016. The overall premium plus estimated out-of-pocket expenses (i.e., deductibles and co-payments) increased 5.1% from 2000-2010 but 2.4% from 2010-2016.
The law is designed to pay aids in the kind of premium tax credits to the individuals or families purchasing the insurance coverage, based on earnings levels. Higher income consumers receive lower subsidies. While pre-subsidy costs rose considerably from 2016 to 2017, so did the aids, to lower the after-subsidy expense to the customer. how much do home health care agencies charge.
However, some or all of these expenses are balanced out by subsidies, paid as tax credits. For instance, the Kaiser Structure reported that for the second-lowest cost "Silver strategy" (a strategy typically selected and utilized as the criteria for figuring out monetary help), a 40-year old non-smoker making $30,000 annually would pay successfully the very same amount in 2017 as they did in 2016 (about $208/month) after the subsidy/tax credit, regardless of large increases in the pre-subsidy cost.
A Health Care Professional Is Caring For A Patient Who Is About To Begin Taking Isoniazid Can Be Fun For Anyone
In other words, the subsidies increased in addition to the pre-subsidy price, fully offsetting the cost boosts. This exceptional tax credit aid is different from the cost sharing reductions subsidy terminated in 2017 by President Donald Trump, an action which raised premiums in the ACA marketplaces by an approximated 20 portion points above what otherwise would have occurred, for the 2018 plan year.
In addition, many workers are choosing to combine a health cost savings account with greater deductible strategies, making the impact of the ACA challenging to identify specifically. For those who acquire their insurance through their employer (" group market"), a 2016 survey found that: Deductibles grew by 63% from 2011 to 2016, while premiums increased 19% and employee incomes grew by 11%.
For firms with less than 200 employees, the deductible averaged $2,069. The portion of employees with a deductible of at least $1,000 grew from 10% in 2006 to 51% in 2016. The 2016 figure drops to 38% after taking employer contributions into account. For the "non-group" market, of which two-thirds are covered by the ACA exchanges, a study of 2015 data discovered that: 49% had private deductibles of a minimum of $1,500 ($ 3,000 for family), up from 36% in 2014.
While about 75% of enrollees were "very pleased" or "rather satisfied" with their option of doctors and health centers, just 50% had such complete satisfaction with their yearly deductible. While 52% of those covered by the ACA exchanges felt "well protected" by their insurance, in the group market 63% felt that way.
prescription drug spending in 2015 was $1,162 per person usually, versus $807 for Canada, $766 for Germany, $668 for France, and $497 for the UK. The factors for higher U.S. healthcare costs relative to http://brooksmapi642.yousher.com/10-easy-facts-about-what-is-a-deductible-in-health-care-explained other countries and gradually are debated by experts. Bar chart comparing healthcare costs as percentage of GDP throughout OECD countries Chart showing life span at birth and healthcare spending per capita for OECD nations as of 2013.
Get This Report about What Does Home Health Care Do
is an outlier, with much greater spending however second-rate life span. U.S. healthcare costs in 2015 were 16.9% GDP according to the OECD, over 5% GDP higher than the next most expensive OECD nation. With U.S. GDP of $19 trillion, health care costs were about $3.2 trillion, or about $10,000 per individual in a country of 320 million people.
In other words, the U.S. would need to cut healthcare expenses by approximately one-third ($ 1 trillion or $3,000 per person on average) to be competitive with the next most expensive country. Health care spending in the U.S. was dispersed as follows in 2014: Healthcare facility care 32%; doctor and medical services 20%; prescription drugs 10%; and all other, including numerous classifications separately comprising less than 5% of costs.
Important distinctions consist of: Administrative expenses. About 25% of U.S. health care costs associate with administrative expenses (e.g., billing and payment, instead of direct arrangement of services, supplies and medication) versus 10-15% in other nations. For example, Duke University Medical facility had 900 medical facility beds but 1,300 billing clerks. Presuming $3.2 trillion is invested on health care per year, a 10% cost savings would be $320 billion each year and a 15% savings would be nearly $500 billion each year.
A 2009 study from Price Waterhouse Coopers approximated $210 billion in cost savings from unneeded billing and administrative expenses, a figure that would be substantially higher in 2015 dollars. Expense variation throughout medical facility regions. Harvard financial expert David Cutler reported in 2013 that roughly 33% of health care costs, or about $1 trillion per year, is not related to improved outcomes.
In 2012, average Medicare repayments per enrollee ranged from a changed (for health status, earnings, and ethnic background) $6,724 in the most affordable costs area to $13,596 in the highest. The U.S. spends more than other nations for the exact same things. Drugs are more pricey, physicians are paid more, and providers charge more for medical equipment than other countries.
Little Known Questions About How To Qualify For Home Health Care.
costs on physicians per individual is about 5 times greater than peer countries, $1,600 versus $310, as much as 37% of the gap with other nations. This was driven by a greater usage of professional physicians, who charge 3-6 times more in the U.S. than in peer countries. Greater level of per-capita earnings, which is associated with higher healthcare spending in the U.S.
Hixon reported a research study by Princeton Professor Uwe Reinhardt that concluded about $1,200 per individual (in 2008 dollars) or about a 3rd of the space with peer countries in healthcare costs was because of higher levels of per-capita earnings. Higher income per-capita is correlated with utilizing more systems of healthcare.
The U.S. takes in 3 times as numerous mammograms, 2.5 x the number of MRI scans, and 31% more C-sections per-capita than peer countries. This is a mix of greater per-capita earnings and higher use of professionals, among other factors. The U.S. government intervenes less actively to require down rates in the United States than in other nations.


Facts About Which Of The Following Are Characteristics Of The Medical Care Determinants Of Health? Uncovered
But cases are accelerating in the U.S., which has become the global epicenter for the infection, with roughly 6 million verified cases and 183,000 deaths or the equivalent of one in 5 COVID-19 fatalities worldwide. "It's actually frustrating to have to divert so much political energy towards what must be a no-brainer." One strength of the Canadian system to shine through during the pandemic is that everybody is insured, Martin said.
Hospitals work with a single insurance company, she stated, and that suggests care is much better collaborated throughout organizations. "Anybody that needs COVID care is going to get it," she stated. Dr. Ashish Jha, who has actually directed the Harvard Global Health Institute and now functions as the dean of the Brown University School of Public Health, has a somewhat various take.
and Canada present "a reflection that has absolutely nothing to do with the underlying health system" however rather shows leaders and their political will and concerns. While America's healthcare system is among the world's finest in regards to development and innovation, Jha said that U.S. political leaders have shown themselves to be reluctant to compromise short-term pain of lockdowns and job losses for a long-lasting public health crisis and economic instability.
They likewise didn't ramp up testing quickly enough to successfully monitor when and where break outs would happen and repeatedly weakened the public health neighborhood in its efforts to efficiently respond to the infection. He said leaders in the U.S. have actually not provided a clear consistent message or decisive management to unify the nation and get everybody relocating the exact same direction.
" It's truly frustrating to have to divert a lot political energy towards what must be a no-brainer," Jha said. "This is the time when everyone who requires to be evaluated, is tested everyone who requires to be taken care of is taken care of." Which begins with consistent access to efficient healthcare, he said.
Not known Incorrect Statements About What Is Single Payer Health Care

entered lockdown under coronavirus, Sen. Bernie Sanders revealed on April 8 that he had ended on his governmental run. A week later on he endorsed former Vice President Joe Biden. After contests in 28 states and two territories, his path to winning the Democratic election had narrowed considerably regardless of an early edge.

His campaign has actually proposed offering "every American a new choice, a public health choice like Medicare" to make insurance more budget friendly. As Potter watches COVID-19 rage in the U.S., the former healthcare communications executive stated Americans reside in "worry of having big out-of-pocket bills without assurance that we'll have our expenditures covered." With the number of uninsured Americans nearly double what they were prior to novel coronavirus, according to some estimates, Potter said that is not sustainable.
response to the coronavirus pandemic was below average, if not the worst, in the world. This pandemic might bring the country to a breaking point, Potter stated, pressing more Americans to call for a health care system that goes beyond the reforms of the Affordable Care Act, which the Trump administration has repeatedly attacked and tried to take apart.
" You will see this campaign resurface to try to terrify people far from change," he said. "It happens whenever there is a considerable push to change the healthcare system. The industry wishes to secure the status quo." There's no perfect health care system, and the Canadian system is not without flaws, Flood said.
In June 2019, New Democrat Celebration Leader Jagmeet Singh proposed expanding Canada's pharmaceutical drug coverage. The ultimate goal of these modifications that have actually been discussed in varying degrees for years is to encompass oral, vision, hearing, psychological health and long-term care to produce "a head to toe healthcare system." And yet it is natural for Canadians to compare systems with their neighbors and merely "feel grateful for what they have (how to take care of your mental health)." She states that type of complacency has insulated Canada's system from further enhancements that produce usually better outcomes for lower expenses, as in the UK, the Netherlands or Switzerland.
10 Simple Techniques For How To Take Care Of Your Mental Health
Healthcare reform has actually been an ongoing argument in the U.S. for years. 2 terms that are typically used in the conversation are universal health care coverage and a single-payer system. They're not the exact same thing, in spite of the fact that individuals often utilize them interchangeably. what is health care fsa. While single-payer systems typically consist of universal coverage, many nations have achieved universal coverage without using a single-payer system.
Universal coverage describes a healthcare system where every individual has health protection. According to the U.S. Census Bureau, there were 28.1 million Americans without medical insurance in 2016, a sharp decrease from the 46.6 million who had actually been uninsured prior to the implementation https://postheaven.net/cassink378/the-population-of-tamil-nadu-has-considerably-benefited-for-example-from-its of the Affordable Care Act (ACA).
Thus, Canada has universal healthcare protection, while the United States does not. It is necessary to note, however, that the 28.5 million uninsured in the U.S. consists of a significant variety of undocumented immigrants. Canada's government-run system does not offer protection to undocumented immigrants. On the other hand, asingle-payer system is one in which there is one entityusually the federal government accountable for paying healthcare claims.
So although it's a kind of government-funded health coverage, the funding originates from two sources rather than one. Individuals who are covered under employer-sponsored health strategies or private market health plans in the U.S. (consisting of ACA-compliant plans) are not part of a single-payer system, and their health insurance coverage is not government-run.
There are presently a minimum of 16 nations that provide some type of a single-payer system, consisting of Canada, Norway, Japan, Spain, the United Kingdom, Portugal, Sweden, Brunei, and Iceland. For the most part, universal protection and a single-payer system go hand-in-hand, because a nation's federal government is the most likely prospect to administer and spend for a health care system covering millions of people.
The 6-Minute Rule for What Is Single Payer Health Care Pros And Cons
However, it is really possible to have universal coverage without having a complete single-payer system, and various nations all over the world have actually done so. Some nations run a in which the federal government supplies standard healthcare with secondary coverage available for those can manage a higher requirement of care. Denmark, France, Australia, Ireland, Hong Kong, Singapore, and Israel each have two-tier systems.
Socialized medication is another expression that is typically discussed in conversations about universal protection, but this design really takes the single-payer system one action even more - which of the following is not a result of the commodification of health care?. In a socialized medicine system, the federal government not only pays for health care but operates the medical facilities and utilizes the medical staff. In the United States, the Veterans Administration (VA) is an example of mingled medicine.
However in Canada, which also has a single-payer system with universal coverage, the healthcare facilities are privately run and doctors are not utilized by the federal government. they just bill the government for the services they offer. The main barrier to any socialized medication system is the federal government's capability to efficiently fund, manage, and upgrade its requirements, equipment, and practices to provide optimal health care.

Fascination About What Is A Health Care Spending Account
An estimated 155 million persons under the age 65 were covered under medical insurance prepares provided by their employers in 2016. The Congressional Spending Plan Office (CBO) estimated that the health insurance premium for single protection would be $6,400 and household coverage would be $15,500 in 2016. The yearly rate of increase in premiums has actually usually slowed after 2000, as part of the trend of lower annual health care expense increases.
This aid encourages people to purchase more substantial protection (which places upward pressure typically premiums), while likewise motivating more young, healthy individuals to enlist (which positions downward pressure on premium prices). CBO estimates the net result is to increase premiums 10-15% over an un-subsidized level. The Kaiser Family Foundation approximated that family insurance premiums balanced $18,142 in 2016, up 3% from 2015, with workers paying $5,277 towards that expense and employers covering the remainder.
The President's Council of Economic Advisors (CEA) described how yearly expense boosts have fallen in the company market given that 2000. Premiums for household coverage grew 5.6% from 2000-2010, however 3.1% from 2010-2016. The total premium plus estimated out-of-pocket costs (i.e., deductibles and co-payments) increased 5.1% from 2000-2010 however 2.4% from 2010-2016.
The law is designed to pay subsidies in the kind of superior tax credits to the people or households purchasing the insurance, based upon earnings levels. Higher income consumers receive lower subsidies. While pre-subsidy costs rose considerably from 2016 to 2017, so did the subsidies, to reduce the after-subsidy expense to the consumer. a health care professional is caring for a patient who is taking zolpidem.
Nevertheless, some or all of these expenses are balanced out by subsidies, paid as tax credits. For example, the Kaiser Foundation reported that for the second-lowest cost "Silver strategy" (a plan typically chosen and used as the benchmark for identifying financial support), a 40-year old non-smoker making $30,000 annually would pay effectively the very same quantity in 2017 as they performed in 2016 (about $208/month) after the subsidy/tax credit, regardless of big increases in the pre-subsidy rate.
Getting My Which Type Of Health Care Facility Employs The Most People In The U.s.? To Work
In other words, the subsidies increased together with the pre-subsidy cost, fully offsetting the rate increases. This exceptional tax credit aid is separate from the expense sharing decreases subsidy stopped in 2017 by President Donald Trump, an action which raised premiums in the ACA markets by an approximated 20 percentage points above what otherwise would have happened, for the 2018 strategy year.
In addition, lots of employees are picking to integrate a health savings account with greater deductible plans, making the effect of the ACA challenging to identify exactly. For those who get their insurance through their employer (" group market"), a 2016 study found that: Deductibles grew by 63% from 2011 to 2016, while premiums increased 19% and employee incomes grew by 11%.
For firms with less than 200 staff members, the deductible averaged $2,069. The portion of workers with a deductible of a minimum of $1,000 grew from 10% in 2006 to 51% in 2016. The 2016 figure drops to 38% after taking company contributions into account. For the "non-group" market, of which two-thirds are covered by the ACA exchanges, a study of 2015 information discovered that: 49% had individual deductibles of at least $1,500 ($ 3,000 for family), up from 36% in 2014.

While about 75% of enrollees were "very satisfied" or "somewhat pleased" with their choice of physicians and health centers, only 50% had such satisfaction with their yearly deductible. While 52% of those covered by the ACA exchanges felt "well protected" by their insurance coverage, in the group market 63% felt that way.
prescription drug spending in 2015 was $1,162 per person usually, versus $807 for Canada, $766 for Germany, $668 for France, http://brooksmapi642.yousher.com/10-easy-facts-about-what-is-a-deductible-in-health-care-explained and $497 for the UK. The factors for greater U.S. health care expenses relative to other nations and over time are disputed by professionals. Bar chart comparing healthcare expenses as percentage of GDP throughout OECD nations Chart showing life span at birth and health care spending per capita for OECD countries since 2013.
How Does The Nurse Manager Or Leader Play A Role In The Reengineering Of Health Care? Things To Know Before You Get This
is an outlier, with much higher costs but below par life span. U.S. healthcare expenses in 2015 were 16.9% GDP according to the OECD, over 5% GDP higher than the next most pricey OECD nation. With U.S. GDP of $19 trillion, healthcare expenses were about $3.2 trillion, or about $10,000 per person in a country of 320 million people.
To put it simply, the U.S. would have to cut healthcare costs by approximately one-third ($ 1 trillion or $3,000 per individual on average) to be competitive with the next most expensive country. Health care spending in the U.S. was dispersed as follows in 2014: Medical facility care 32%; physician and medical services 20%; prescription drugs 10%; and all other, including many classifications separately comprising less than 5% of costs.
Crucial distinctions include: Administrative costs. About 25% of U.S. health care expenses connect to administrative costs (e.g., billing and payment, instead of direct provision of services, products and medicine) versus 10-15% in other countries. For instance, Duke University Healthcare facility had 900 hospital beds however 1,300 billing clerks. Assuming $3.2 trillion is invested in healthcare annually, a 10% savings would be $320 billion per year and a 15% savings would be almost $500 billion annually.
A 2009 study from Price Waterhouse Coopers estimated $210 billion in savings from unnecessary billing and administrative expenses, a figure that would be considerably greater in 2015 dollars. Cost variation throughout hospital areas. Harvard economic expert David Cutler reported in 2013 that approximately 33% of health care spending, or about $1 trillion per year, is not connected with enhanced outcomes.
In 2012, typical Medicare reimbursements per enrollee varied from a changed (for health status, earnings, and ethnic culture) $6,724 in the most affordable spending area to $13,596 in the highest. The U.S. spends more than other nations for the exact same things. Drugs are more expensive, doctors are paid more, and suppliers charge more for medical devices than other nations.
Which Of The Following Is Not A Result Of The Commodification Of Health Care for Beginners

spending on physicians per individual is about five times higher than peer countries, $1,600 versus $310, as much as 37% of the space with other nations. This was driven by a greater use of expert doctors, who charge 3-6 times more in the U.S. than in peer countries. Higher level of per-capita earnings, which is correlated with higher health care spending in the U.S.
Hixon reported a research study by Princeton Professor Uwe Reinhardt that concluded about $1,200 per individual (in 2008 dollars) or about a third of the space with peer countries in healthcare spending was because of higher levels of per-capita income. Higher income per-capita is correlated with utilizing more units of healthcare.
The U.S. consumes 3 times as many mammograms, 2.5 x the number of MRI scans, and 31% more C-sections per-capita than peer countries. This is a mix of greater per-capita income and higher usage of professionals, among other elements. The U.S. federal government intervenes less actively to require down costs in the United States than in other nations.

3 Simple Techniques For Which Of The Following Represents The Status Of A Right To Health Care In The United States?
But cases are accelerating in the U.S., which has ended up being the international epicenter for the infection, with roughly 6 million verified cases and 183,000 deaths or the equivalent of one in 5 COVID-19 casualties worldwide. "It's truly aggravating to need to divert so much political energy towards what must be a no-brainer." One strength of the Canadian system to shine through during the pandemic is that everybody is insured, Martin stated.
Medical facilities work with a single insurance provider, she stated, which suggests care is better collaborated across organizations. "Anyone that requires COVID care is going to get it," she stated. Dr. Ashish Jha, who has directed the Harvard Global Health Institute and now functions as the dean of the Brown University School of Public Health, has a slightly various take.
and Canada present "a reflection that has nothing to do with the underlying health system" but rather reflects leaders and their political will and concerns. While America's health care system is among the world's finest in terms of development and innovation, Jha stated that U.S. politicians have shown themselves to be reluctant to trade off short-term discomfort of lockdowns and task losses for a long-term public health https://postheaven.net/cassink378/the-population-of-tamil-nadu-has-considerably-benefited-for-example-from-its crisis and financial instability.
They also didn't increase testing quickly enough to successfully monitor when and where outbreaks would occur and repeatedly weakened the public health community in its efforts to effectively react to the virus. He stated leaders in the U.S. have actually not offered a clear consistent message or definitive leadership to join the country and get everybody moving in the very same direction.
" It's actually aggravating to have to divert so much political energy towards what ought to be a no-brainer," Jha said. "This is the time when everybody who needs to be tested, is tested everyone who requires to be taken care of is looked after." And that starts with uniform access to effective healthcare, he said.
The Best Guide To What Is Required In The Florida Employee Health Care Access Act?
entered lockdown under coronavirus, Sen. Bernie Sanders announced on April 8 that he had ended on his governmental run. A week later he backed previous Vice President Joe Biden. After contests in 28 states and two territories, his path to winning the Democratic election had narrowed significantly regardless of an early edge.
His campaign has proposed using "every American a new choice, a public health choice like Medicare" to make insurance coverage more budget-friendly. As Potter watches COVID-19 rage in the U.S., the former health care communications executive said Americans live in "fear of having big out-of-pocket expenses without guarantee that we'll have our expenses covered." With the number of uninsured Americans almost double what they were prior to novel coronavirus, according to some estimates, Potter said that is not sustainable.
reaction to the coronavirus pandemic was below par, if not the worst, on the planet. This pandemic could bring the country to a snapping point, Potter said, pushing more Americans to require a health care system that exceeds the reforms of the Affordable Care Act, which the Trump administration has actually consistently assaulted and attempted to dismantle.

" You will see this project resurface to try to scare people away from change," he said. "It takes place whenever there is a substantial push to change the health care system. The market wishes to safeguard the status quo." There's no perfect health care system, and the Canadian system is not without flaws, Flood said.
In June 2019, New Democrat Party Leader Jagmeet Singh proposed broadening Canada's pharmaceutical drug protection. The ultimate goal of these changes that have actually been disputed in differing degrees for many years is to incorporate dental, vision, hearing, mental health and long-term care to produce "a head to toe health care system." And yet it is natural for Canadians to compare systems with their next-door neighbors and simply "feel grateful for what they have (what countries have universal health care)." She says that type of complacency has actually insulated Canada's system from further enhancements that produce generally much better results for lower expenses, as in the UK, the Netherlands or Switzerland.

Not known Details About What Is Single Payer Health Care
Health care reform has actually been an ongoing argument in the U.S. for decades. Two terms that are often used in the conversation are universal healthcare protection and a single-payer system. They're not the very same thing, despite the truth that people sometimes use them interchangeably. what is fsa health care. While single-payer systems normally include universal protection, many countries have accomplished universal protection without utilizing a single-payer system.
Universal coverage refers to a healthcare system where every person has health protection. According to the U.S. Census Bureau, there were 28.1 million Americans without medical insurance in 2016, a sharp decrease from the 46.6 million who had actually been uninsured prior to the execution of the Affordable Care Act (ACA).
Hence, Canada has universal healthcare coverage, while the United States does not. It is very important to keep in mind, however, that the 28.5 million uninsured in the U.S. includes a considerable number of undocumented immigrants. Canada's government-run system does not offer protection to undocumented immigrants. On the other hand, asingle-payer system is one in which there is one entityusually the federal government accountable for paying health care claims.
So although it's a type of government-funded health coverage, the funding comes from two sources instead of one. People who are covered under employer-sponsored health insurance or individual market health plans in the U.S. (including ACA-compliant strategies) are not part of a single-payer system, and their medical insurance is not government-run.
There are currently at least 16 countries that provide some kind of a single-payer system, consisting of Canada, Norway, Japan, Spain, the UK, Portugal, Sweden, Brunei, and Iceland. In many cases, universal protection and a single-payer system go hand-in-hand, because a country's federal government is the most likely prospect to administer and pay for a health care system covering countless people.
Getting The How To Start A Home Health Care Agency To Work
Nevertheless, it is extremely possible to have universal protection without having a complete single-payer system, and numerous countries around the globe have actually done so. Some nations operate a in which the federal government supplies basic healthcare with secondary coverage offered for those can pay for a greater requirement of care. Denmark, France, Australia, Ireland, Hong Kong, Singapore, and Israel each have two-tier systems.
Interacted socially medicine is another expression that is often mentioned in conversations about universal coverage, however this model actually takes the single-payer system one step even more - who is eligible for care within the veterans health administration. In a socialized medication system, the federal government not only spends for health care however operates the hospitals and employs the medical staff. In the United States, the Veterans Administration (VA) is an example of socialized medicine.
However in Canada, which likewise has a single-payer system with universal protection, the medical facilities are independently operated and doctors are not used by the government. they just bill the government for the services they supply. The main barrier to any socialized medicine system is the government's capability to successfully fund, handle, and upgrade its requirements, devices, and practices to offer ideal healthcare.

The Best Strategy To Use For Which Team Member Acts As A Liaison Between The Health Care Facility And The Media?
Their healthcare advantages consist of healthcare facility care, main care, prescription drugs, and conventional Chinese medication. However not everything is covered, including pricey treatments for rare illness. Patients need to make copays when they see a physician, check out the ED, or fill a prescription, but the expense is typically less than about $12, and varies based upon patient earnings.
Still, it may spread physicians too thin, Vox reports: In Taiwan, the average number of doctor check outs each year is currently 12.1, which is almost twice the variety of gos to in other established economies. In addition, there are just about 1.7 doctors for each 1,000 patientsbelow the average of 3.3 in other industrialized nations.
As an outcome, Taiwanese doctors usually work about 10 more hours each week than U.S. doctors. Physician compensation can likewise be a problem, Scott reports. One physician said the requiring nature of his pediatric practice led him to practice cosmetic medicinewhich is more rewarding and paid privately by patientson the side, Vox reports.
For example, clients note they experience hold-ups in accessing new medical treatments under the nation's health system. Sometimes, Taiwanese clients wait five years longer than U.S. clients to access the most recent treatments. Taiwan's rating on the HAQ Index shows the significant improvement in health outcomes among Taiwanese residents because the single-payer design's application.
But while Taiwanese homeowners are living longer, the system's effect on doctors and growing expenses provides obstacles and raises concerns about the system's financial substantiality, Scott reports. The U.K. health system offers health care through single-payer model that is both financed and run by the federal government. The outcome, as Vox's Ezra Klein reports, is a system in which "rationing isn't an unclean word." The U.K.'s system is funded through taxes and administered through the (NHS), which was established in 1948.
produced the (GREAT) to identify the cost-effectiveness of treatments NHS thinks about covering. GOOD makes its protection decisions utilizing a metric called the QALY, which is brief for quality-adjusted life years. Usually, treatments with a QALY listed below $26,000 per year will receive NICE's approval for coverage - how does universal health care work. The decision is less certain for treatments where a QALY is between $26,000 and $40,000, and drugs with a QALY above $40,000 are not likely to get approval, according to Klein.
NICE has actually dealt with particular criticism over its approval process for brand-new costly cancer drugs, resulting in the establishment of a public fund to assist cover the expense of these drugs. U.K. citizens covered by NHS do not pay premiums and instead contribute to the health system via taxes. Patients can acquire additional private insurance coverage, however they hardly ever do so: Only about 10% of residents purchase personal protection, Klein reports.
6 Easy Facts About What Is The New Health Care Plan Explained
citizens are less most likely to avoid essential care since of costswith 33% of U.S. residents reporting they've done so, while just 7% of U.K. residents stated they did the very same. However that's not state U.K. residents do not face difficulties getting a medical professional's appointment. U.K. residents are three times as most likely as Americans to say that had to wait over 3 months for an expert consultation.
concerning NICE's handling of specific cancer drugs. According to Klein, "reaction to NICE's rejections [of the cancer drugs] and slow-moving procedure" resulted in the creation of a different public fund to cover cancer drugs that NICE hasn't approved or assessed. The U.K. scores 90.5 on HAQ index, higher than the United States but lower than Australia.
system is "underfunded," research study has revealed that residents largely support the system." [GOOD] has actually made the UK system distinctively centralized, transparent, and fair," Klein composes. "However it is developed on a faith in federal government, and a political Additional reading and social uniformity, that is difficult to think of in the United States."( Scott, Vox, 1/15; Scott, Vox, 1/17; Scott, Vox, 1/13; Scott, Vox, 1/29; Klein, Vox, 1/28; The Lancet, accessed 2/13).
Naresh Tinani enjoys his job as a perfusionist at a health center in beaufokl680.huicopper.com/the-definitive-guide-for-why-is-health-care-so-expensive Saskatchewan's capital. To him, monitoring client blood levels, heart beat and body temperature throughout cardiac surgical treatments and extensive care is a "opportunity" "the supreme interaction between human physiology and the mechanics of engineering." But Tinani has likewise been on the opposite of the system, like when his now-15-year-old twin children were born 10 weeks early and fought infection on life assistance, or as his 78-year-old mother waits months for new knees in the middle of the coronavirus pandemic.
He's proud due to the fact that throughout times of real emergency, he stated the system looked after his family without adding expense and affordability to his list of worries. And on that point, few Americans can say the same. Prior to the coronavirus pandemic hit the U.S. complete speed, fewer than half of Americans 42 percent considered their health care system to be above average, according to a PBS NewsHour/Marist poll performed in late July.
Compared to people in many established nations, including Canada, Americans have for years paid even more for healthcare while remaining sicker and dying sooner. In the United States, unlike many nations in the industrialized world, medical insurance is frequently tied to whether or not you have a task. More than 160 million Americans depend on their companies for medical insurance prior to COVID-19, while another 30 million Americans lacked medical insurance prior to the pandemic.
Numbers are still shaking out, but one projection from the Urban Institute and the Robert Wood Johnson Foundation recommended as numerous as 25 million more Americans became uninsured in recent months. That research study recommended that countless Americans will fall through the fractures and might stop working to enlist for Medicaid, the country's safeguard healthcare program, which covered 75 million people prior to the pandemic.

The Facts About Who Health Care Rankings Uncovered
Check just how much you know with this test. When people dispute how to repair the damaged U.S. system (a specifically common discussion throughout governmental election years), Canada invariably turns up both as an example the U.S. need to appreciate and as one it must prevent. Throughout the 2020 Democratic primary season, Sen.
health care system, pitching his own variation called "Medicare for All." Sanders leaving of the race in April fueled speculation that Biden may embrace a more progressive platform, consisting of on health care, to charm Sanders' diehard fans. Every healthcare system has its strengths and weak points, including Canada's. Here's how that nation's system works, why it's admired (and sometimes disparaged) by some in the U.S., and why results in the 2 nations have been so different throughout the COVID-19 pandemic.
In 1944, citizens in the rural province of Saskatchewan, hard-hit throughout the Great Anxiety, elected a democratic socialist government after political leaders had actually campaigned for a fundamental right to healthcare. At the time, people felt "that the system simply wasn't working" and they wanted to attempt something different, said Greg Marchildon, a health care historian who teaches health policy and systems at the University of Toronto.
The change was met pushback. On July 1, 1962, medical professionals staged a 23-day strike in the provincial capital of Regina to object universal health coverage. However ultimately, the program "had actually ended up being popular enough that it would end up being too politically harming Click here for more to take it away," Marchildon stated. Other provinces took notification.

The Ultimate Guide To What Is Health Care Administration
Their health care advantages include hospital care, primary care, prescription drugs, and traditional Chinese medication. However not everything is covered, including costly treatments for rare diseases. Patients need to make copays when they see a physician, go to the ED, or fill a prescription, however the expense is typically less than about $12, and differs based upon patient income.
Still, it may spread medical professionals too thin, Vox reports: In Taiwan, the average variety of physician visits each year is currently 12.1, which is almost twice the number of visits in other established economies. In addition, there are only about 1.7 doctors for every 1,000 patientsbelow the average of 3.3 in other industrialized nations.
As a result, Taiwanese doctors on typical work about 10 more hours each week than U.S. doctors. Doctor settlement can also be a problem, Scott reports. One doctor said the demanding nature of his pediatric practice led him to practice cosmetic medicinewhich is more lucrative and paid privately by patientson the side, Vox reports.
For example, patients note they experience hold-ups in accessing new medical treatments under the nation's health system. Often, Taiwanese patients wait five years longer than U.S. clients to access the most recent treatments. Taiwan's score on the HAQ Index reveals the significant enhancement in health outcomes amongst Taiwanese homeowners given that the single-payer model's implementation.
But while Taiwanese locals are living longer, the system's impact on physicians and growing expenses provides challenges and raises questions about the system's financial substantiality, Scott reports. The U.K. health system provides health care through single-payer design that is both funded and run by the federal government. The outcome, as Vox's Ezra Klein reports, is a system in which "rationing isn't a dirty word." The U.K.'s system is moneyed through taxes and administered through the (NHS), which was developed in 1948.
created the (GREAT) to figure out the cost-effectiveness of treatments NHS thinks about covering. GOOD makes its coverage choices using a metric understood as the QALY, which is brief for quality-adjusted life years. Normally, treatments with a QALY below $26,000 per year will receive NICE's approval for protection - how much is health care. The choice is less specific for treatments where a QALY is in between $26,000 and $40,000, and drugs with a QALY above $40,000 are unlikely to get approval, according to Klein.
NICE has faced particular criticism over its approval process for brand-new expensive cancer drugs, resulting in the establishment of a public fund to help cover the cost of these drugs. U.K. homeowners covered by NHS do not pay premiums and rather contribute to the health system by means of taxes. Patients can buy additional personal insurance, however they rarely do so: Only about 10% of citizens purchase private protection, Klein reports.
Click here for more style="clear:both" id="content-section-1">Not known Details About How Many Countries Have Universal Health Care
citizens are less likely to skip necessary care because of costswith 33% of U.S. homeowners reporting they've done so, while just 7% of U.K. citizens said they did the very same. However that's not say U.K. locals do not face difficulties getting a medical professional's visit. U.K. residents are 3 times as most likely as Americans to say that had to wait over 3 months for a professional visit.
regarding NICE's handling of certain cancer drugs. According to Klein, "reaction to NICE's rejections [of the cancer drugs] and slow-moving process" resulted in the creation of a separate public fund to cover cancer drugs that NICE hasn't approved or examined. The U.K. scores 90.5 on HAQ index, higher than beaufokl680.huicopper.com/the-definitive-guide-for-why-is-health-care-so-expensive the United States however lower than Australia.

system is "underfunded," research has shown that citizens largely support the system." [GREAT] has actually made the UK system distinctively centralized, transparent, and equitable," Klein composes. "But it is constructed on a faith in federal government, and a political and social solidarity, that is tough to imagine in the US."( Scott, Vox, 1/15; Scott, Vox, 1/17; Scott, Vox, 1/13; Scott, Vox, 1/29; Klein, Vox, 1/28; The Lancet, accessed 2/13).
Naresh Tinani loves his job as a perfusionist at a hospital in Saskatchewan's capital. To him, monitoring patient blood levels, heart beat and body temperature level during heart surgical treatments and intensive care is a "advantage" "the supreme interaction in between human physiology and the mechanics of engineering." However Tinani has also been on the opposite of the system, like when his now-15-year-old twin children were born 10 weeks early and battled infection on life assistance, or as his 78-year-old mom waits months for new knees amid the coronavirus pandemic.
He's proud because throughout times of real emergency situation, he stated the system looked after his family without adding cost and price to his list of worries. And on that point, couple of Americans can state the very same. Before the coronavirus pandemic struck the U.S. complete speed, fewer than half of Americans 42 percent considered their healthcare system to be above average, according to a PBS NewsHour/Marist poll conducted in late July.
Compared to people in the majority of established nations, consisting of Canada, Americans have for years paid even Additional reading more for health care while remaining sicker and dying quicker. In the United States, unlike most countries in the developed world, health insurance coverage is often connected to whether or not you have a job. More than 160 million Americans count on their companies for medical insurance prior to COVID-19, while another 30 million Americans were without health insurance coverage prior to the pandemic.
Numbers are still shaking out, but one projection from the Urban Institute and the Robert Wood Johnson Structure suggested as numerous as 25 million more Americans ended up being uninsured in recent months. That research study recommended that millions of Americans will fall through the cracks and may fail to enroll for Medicaid, the country's safeguard health care program, which covered 75 million people before the pandemic.
The smart Trick of What Does A Health Care Administration Do That Nobody is Talking About
Check how much you know with this test. When individuals discuss how to fix the damaged U.S. system (a specifically common discussion throughout presidential election years), Canada inevitably comes up both as an example the U.S. should appreciate and as one it ought to prevent. During the 2020 Democratic main season, Sen.
healthcare system, pitching his own version called "Medicare for All." Sanders leaving of the race in April fueled speculation that Biden might embrace a more progressive platform, including on health care, to woo Sanders' diehard advocates. Every healthcare system has its strengths and weak points, consisting of Canada's. Here's how that nation's system works, why it's appreciated (and sometimes disparaged) by some in the U.S., and why outcomes in the two nations have actually been so various during the COVID-19 pandemic.
In 1944, citizens in the rural province of Saskatchewan, hard-hit during the Great Anxiety, chose a democratic socialist government after political leaders had actually campaigned for a basic right to health care. At the time, people felt "that the system simply wasn't working" and they were prepared to attempt something different, said Greg Marchildon, a health care historian who teaches health policy and systems at the University of Toronto.
The modification was fulfilled with pushback. On July 1, 1962, physicians staged a 23-day strike in the provincial capital of Regina to oppose universal health protection. But ultimately, the program "had actually ended up being popular enough that it would become too politically damaging to take it away," Marchildon said. Other provinces took notification.

The Single Strategy To Use For What Countries Have Universal Health Care
Their health care advantages include hospital care, primary care, prescription drugs, and standard Chinese medication. However not everything is covered, consisting of pricey treatments for rare illness. Clients have to make copays when they see a physician, check out the ED, or fill a prescription, but the expense is typically less than about $12, and varies based upon client income.
Still, it may spread out medical professionals too thin, Vox reports: In Taiwan, the average number of physician visits each year is currently 12.1, which is nearly twice the variety of sees in other established economies. In addition, there are just about 1.7 physicians for every single 1,000 patientsbelow the average of 3.3 in other industrialized countries.
As an outcome, Taiwanese physicians on typical work about 10 more hours weekly than U.S. doctors. Physician payment can also be a problem, Scott reports. One physician stated the demanding nature of his pediatric practice led him to practice cosmetic medicinewhich is more lucrative and paid independently by patientson the side, Vox reports.
For circumstances, patients note they experience hold-ups in accessing new medical treatments under the country's health system. In some cases, Taiwanese patients wait 5 years longer than U.S. patients to access the most recent treatments. Taiwan's score on the HAQ Index reveals the significant improvement in health outcomes amongst Taiwanese locals since the single-payer design's execution.
However while Taiwanese homeowners are living longer, the system's influence on doctors and growing expenses provides challenges and raises concerns about the system's financial substantiality, Scott reports. The U.K. health system offers healthcare through single-payer model that is both funded and run by the federal government. The result, as Vox's Ezra Klein reports, is a system in which "rationing isn't a dirty word." The U.K.'s system is funded through taxes and administered through the (NHS), which was established Additional reading in 1948.
produced the (NICE) to figure out the cost-effectiveness of treatments NHS thinks about covering. GOOD makes its coverage decisions utilizing a metric called the QALY, which is brief for quality-adjusted life years. Usually, treatments with a QALY listed below $26,000 per year will receive NICE's approval for protection - what is health care fsa. The decision is less particular for treatments where a QALY is in between $26,000 and $40,000, and drugs with a QALY above $40,000 are unlikely to get approval, according to Klein.
NICE has beaufokl680.huicopper.com/the-definitive-guide-for-why-is-health-care-so-expensive actually dealt with particular criticism over its approval process for brand-new pricey cancer drugs, resulting in the facility of a public fund to assist cover the cost of these drugs. U.K. locals covered by NHS do not pay premiums and instead add to the health system through taxes. Clients can acquire supplemental personal insurance coverage, however they rarely do so: Just about 10% of homeowners purchase private protection, Klein reports.
Not known Details About Identify The Reasons Why Doctors Wield Power In Today’s Health Care System.
residents are less likely to skip necessary care since of costswith 33% of U.S. homeowners reporting they've done so, while only 7% of U.K. citizens said they did the very same. However that's not state U.K. locals do not face hardships getting a medical professional's visit. U.K. locals are three times as likely as Americans to state that had to wait over 3 months for a specialist appointment.
relating to NICE's handling of specific cancer drugs. According to Klein, "backlash to NICE's rejections [of the cancer drugs] and slow-moving process" led to the creation of a different public fund to cover cancer drugs that NICE hasn't authorized or evaluated. The U.K. ratings 90.5 on HAQ index, higher than the United States however lower than Australia.
system is "underfunded," research has actually revealed that locals mostly support the system." [NICE] has actually made the UK system uniquely centralized, transparent, and equitable," Klein composes. "But it is developed on a faith in government, and a political and social solidarity, that is tough to picture in the United States."( Scott, Vox, 1/15; Scott, Vox, 1/17; Scott, Vox, 1/13; Scott, Vox, 1/29; Klein, Vox, 1/28; The Lancet, accessed 2/13).
Naresh Tinani loves his job as a perfusionist at a hospital in Saskatchewan's capital. To him, keeping track of patient blood levels, heart beat and body temperature level during heart surgical treatments and extensive care is a "advantage" "the supreme interaction between human physiology and the mechanics of engineering." But Tinani has actually likewise been on the opposite of the system, like when his now-15-year-old twin children were born 10 weeks early and fought infection on life assistance, or as his 78-year-old mother waits months for brand-new knees amid the coronavirus pandemic.
He's proud due to the fact that during times of true emergency situation, he stated the system looked after his Click here for more family without including cost and cost to his list of concerns. And on that point, couple of Americans can state the very same. Before the coronavirus pandemic struck the U.S. full speed, less than half of Americans 42 percent considered their health care system to be above average, according to a PBS NewsHour/Marist survey conducted in late July.
Compared to individuals in most developed countries, consisting of Canada, Americans have for years paid far more for health care while remaining sicker and passing away faster. In the United States, unlike most countries in the industrialized world, health insurance coverage is frequently connected to whether or not you have a job. More than 160 million Americans depend on their companies for medical insurance prior to COVID-19, while another 30 million Americans were without health insurance prior to the pandemic.
Numbers are still cleaning, however one projection from the Urban Institute and the Robert Wood Johnson Foundation suggested as many as 25 million more Americans became uninsured in current months. That study suggested that countless Americans will fail the cracks and might stop working to register for Medicaid, the country's safety net health care program, which covered 75 million people before the pandemic.
The Best Guide To Which Of The Following Frequently Causes Health-care-associated Infections Of The Gi Tract?
Test how much you understand with this test. When individuals discuss how to fix the broken U.S. system (a particularly typical discussion during governmental election years), Canada invariably shows up both as an example the U.S. need to admire and as one it must prevent. Throughout the 2020 Democratic main season, Sen.
healthcare system, pitching his own version called "Medicare for All." Sanders leaving of the race in April fueled speculation that Biden may adopt a more progressive platform, consisting of on health care, to woo Sanders' diehard fans. Every healthcare system has its strengths and weaknesses, including Canada's. Here's how that nation's system works, why it's appreciated (and in some cases disparaged) by some in the U.S., and why outcomes in the two nations have been so various during the COVID-19 pandemic.
In 1944, voters in the rural province of Saskatchewan, hard-hit during the Great Anxiety, chose a democratic socialist government after politicians had campaigned for a fundamental right to health care. At the time, individuals felt "that the system simply wasn't working" and they were prepared to try something various, said Greg Marchildon, a health care historian who teaches health policy and systems at the University of Toronto.
The modification was met pushback. On July 1, 1962, doctors staged a 23-day strike in the provincial capital of Regina to oppose universal health protection. But eventually, the program "had become popular enough that it would become too politically damaging to take it away," Marchildon said. Other provinces took notice.

The Single Strategy To Use For Who Is The Executive Team At People Care Health Services
However cases are speeding up in the U.S., which has ended up being the international epicenter for the Visit this website infection, with approximately 6 million confirmed cases and 183,000 deaths or the equivalent of one in 5 COVID-19 deaths worldwide. "It's really discouraging to need to divert a lot political energy towards what needs to be a no-brainer." One strength of the Canadian system to shine through throughout the pandemic is that everyone is guaranteed, Martin stated.
Hospitals work with a single insurance company, she said, and that suggests care is much better collaborated across institutions. "Any person that requires COVID care is going to get it," she stated. Dr. Ashish Jha, who has directed the Harvard Global Health Institute and now works as the dean of the Brown University School of Public Health, has a somewhat various take.
and Canada present "a reflection that has absolutely nothing to do with the underlying health system" but rather shows leaders and their political will and concerns. While America's health care system is among the world's best in terms of innovation and innovation, Jha said that U.S. politicians have actually shown themselves to be unwilling to trade off short-term pain of lockdowns and job losses for a long-lasting public health crisis and economic instability.
They also didn't increase screening rapidly enough to successfully keep track of when and where break outs would take place and consistently undermined the general public health community in its efforts to effectively respond to the virus. He stated leaders in the U.S. have not used a clear constant message or definitive leadership to join the country and get everyone moving in the exact same direction.
" It's truly aggravating to need to divert a lot political energy towards what must be a no-brainer," Jha said. "This is the time when everyone who requires to be tested, is tested everyone who requires to be taken care of is taken care of." And that begins with uniform access to effective healthcare, he stated.
More About When Does Senate Vote On Health Care Bill

gotten in lockdown under coronavirus, Sen. Bernie Sanders announced on April 8 that he had actually ended on his governmental run. A week later he endorsed previous Vice President Joe Biden. After contests in 28 states and 2 territories, his course to winning the Democratic nomination had narrowed considerably regardless of an early edge.
His campaign has actually proposed using "every American a new choice, a public health choice like Medicare" to make insurance more inexpensive. As Potter sees COVID-19 rage in the U.S., the previous health care interactions executive said Americans live in "worry of having huge out-of-pocket costs without assurance that we'll have our expenditures covered." With the number of uninsured Americans nearly double what they were prior to unique coronavirus, according to some estimates, Potter stated that is not sustainable.
action to the coronavirus pandemic was listed below average, if not the worst, in the world. This pandemic might bring the country to a snapping point, Potter said, pushing more Americans to require a health care system that exceeds the reforms of the Affordable Care Act, which the Trump administration has consistently attacked and tried to take apart.
" You will see this project resurface to try to frighten individuals far from change," he stated. "It occurs whenever there is a significant push to change the health care system. The market wishes to safeguard the status quo." There's no ideal health care system, and the Canadian system is not without defects, Flood stated.
In June 2019, New Democrat Party Leader Jagmeet Singh proposed expanding Canada's pharmaceutical drug coverage. The eventual objective of these changes that have actually been debated in varying degrees for many years is to include dental, vision, hearing, psychological health and long-term care to create "a head to toe healthcare system." And yet it is natural for Canadians to compare systems with their next-door neighbors and just "feel grateful for what they have (how much does medicare pay for home health care per hour)." She says that type of complacency has actually insulated Canada's system from more improvements that produce typically better outcomes for lower costs, as in the UK, the Netherlands or Switzerland.
Not known Incorrect Statements About Which Type Of Health Insurance Plan Is Not Considered A Managed Care Plan?
Health care reform has been a continuous dispute in the U.S. for decades. 2 terms that are frequently utilized in the conversation are universal healthcare coverage and a single-payer system. They're not the exact same thing, regardless of the reality that individuals sometimes utilize them interchangeably. which of the following are characteristics of the medical care determinants https://telegra.ph/what-does-what-is-the-impact-of-managed-care-on-cost-do-10-21 of health?. While single-payer systems normally consist of universal coverage, many nations have attained universal coverage without using a single-payer system.
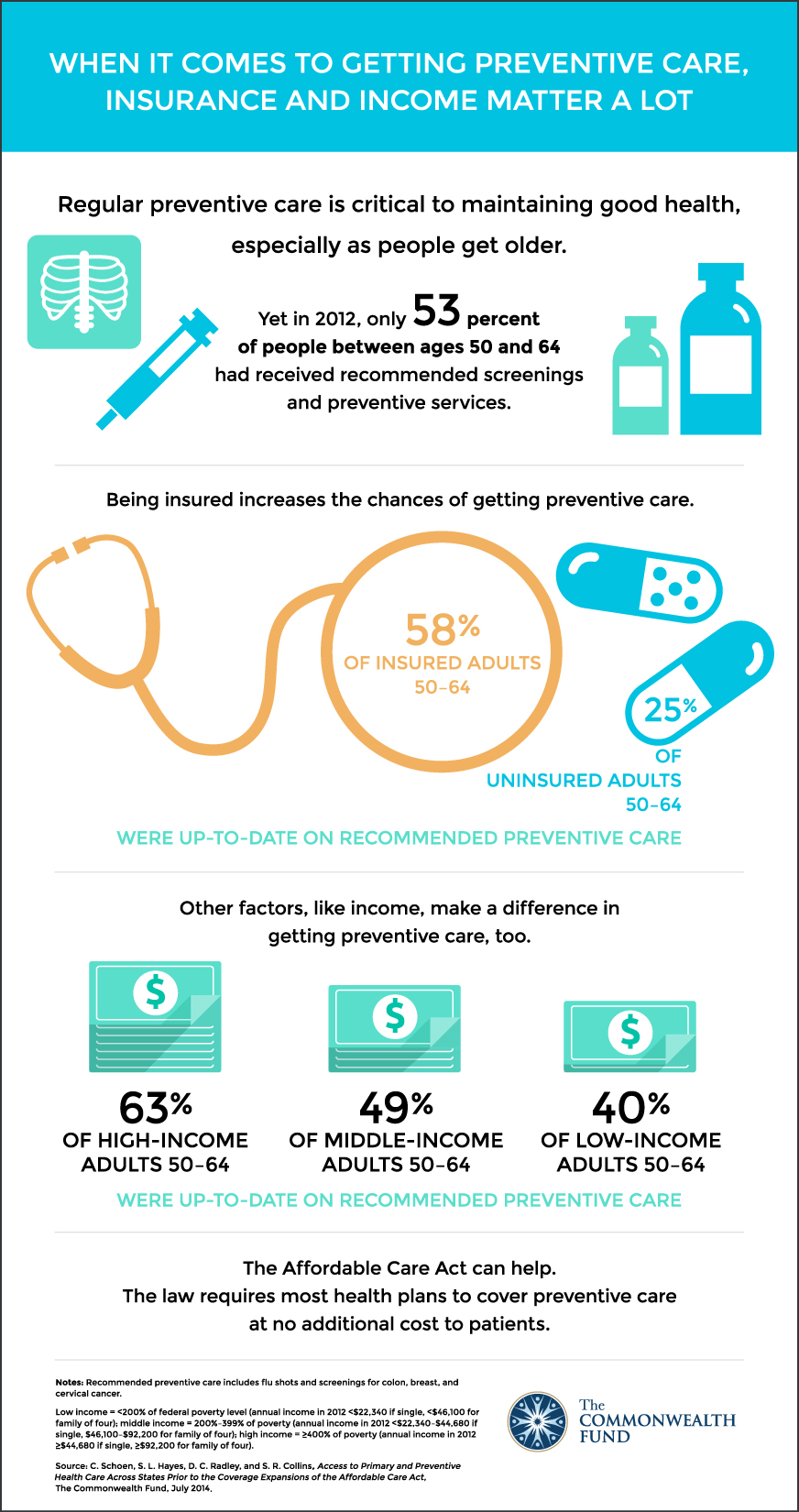
Universal coverage describes a healthcare system where every person has health coverage. According to the U.S. Census Bureau, there were 28.1 million Americans without medical insurance in 2016, a sharp decrease from the 46.6 million who had actually been uninsured prior to the implementation of the Affordable Care Act (ACA).
Hence, Canada has universal health care protection, while the United States does not. It is necessary to keep in mind, however, that the 28.5 million uninsured in the U.S. includes a substantial number of undocumented immigrants. Canada's government-run system does not offer coverage to undocumented immigrants. On the other hand, asingle-payer system is one in which there is one entityusually the government responsible for paying health care claims.
So although it's a form of government-funded health coverage, the funding comes from 2 sources rather than one. Individuals who are covered under employer-sponsored health plans or individual market health insurance in the U.S. (consisting of ACA-compliant plans) are not part of a single-payer system, and their medical insurance is not government-run.
There are currently a minimum of 16 nations that offer some type of a single-payer system, including Canada, Norway, Japan, Spain, the UK, Portugal, Sweden, Brunei, and Iceland. In many cases, universal coverage and a single-payer system go hand-in-hand, since a country's federal government is the most likely prospect to administer and pay for a healthcare system covering countless people.
Getting My How Does The Health Care Tax Credit Affect My Tax Return To Work
However, it is extremely possible to have universal protection without having a full single-payer system, and various nations around the world have actually done so. Some countries operate a in which the government provides basic health care with secondary coverage readily available for those can manage a greater requirement of care. Denmark, France, Australia, Ireland, Hong Kong, Singapore, and Israel each have two-tier systems.
Interacted socially medication is another phrase that is often discussed in conversations about universal coverage, but this model in fact takes the single-payer system one step even more - when does senate vote on health care bill. In a socialized medicine system, the government not only spends for health care however operates the medical facilities and uses the medical personnel. In the United States, the Veterans Administration (VA) is an example of interacted socially medicine.
However in Canada, which likewise has a single-payer system with universal protection, the health centers are privately run and physicians are not employed by the government. they merely bill the federal Addiction Treatment Facility government for the services they provide. The main barrier to any socialized medicine system is the federal government's ability to efficiently money, handle, and update its standards, devices, and practices to offer optimal healthcare.

The 4-Minute Rule for What Is The Role Of Insurance Payers In The Quality Of Services Of A Health Care Organization
But cases are speeding up in the U.S., which has become the worldwide epicenter for the virus, with approximately 6 million confirmed cases and 183,000 deaths or the equivalent of one in 5 COVID-19 deaths worldwide. "It's actually frustrating to need to divert so much political energy towards what should be a no-brainer." One strength of the Canadian system to shine through throughout the pandemic is that everyone is guaranteed, Martin stated.
Medical facilities deal with a single insurance provider, she stated, which implies care is better collaborated throughout organizations. "Anybody that requires COVID care is going to get it," she stated. Dr. Ashish Jha, who has directed the Harvard Global Health Institute and now functions as the dean of the Brown University School https://telegra.ph/what-does-what-is-the-impact-of-managed-care-on-cost-do-10-21 of Public Health, has a somewhat various take.
and Canada present "a reflection that has nothing to do with the underlying Addiction Treatment Facility health system" but rather shows leaders and their political will and top priorities. While America's health care system is amongst the world's finest in terms of innovation and innovation, Jha stated that U.S. politicians have revealed themselves to be unwilling to compromise short-term pain of lockdowns and task losses for a long-lasting public health crisis and economic instability.
They likewise didn't increase testing quickly enough to efficiently monitor when and where outbreaks would take place and consistently weakened the public health community in its efforts to efficiently react to the infection. He stated leaders in the U.S. have actually not offered a clear consistent message or definitive leadership to unify the nation and get everybody relocating the very same direction.
" It's actually discouraging to need to divert so much political energy towards what needs to be a no-brainer," Jha said. "This is the time when everyone who requires to be evaluated, is checked everybody who needs to be taken care of is looked after." Which starts with consistent access to efficient health care, he said.
Things about What Is Preventive Health Care
gotten in lockdown under coronavirus, Sen. Bernie Sanders revealed on April 8 that he had actually ended on his presidential run. A week later on he backed previous Vice President Joe Biden. After contests in 28 states and two areas, his path to winning the Democratic election had actually narrowed significantly despite an early edge.
His project has proposed providing "every American a brand-new option, a public health choice like Medicare" to make insurance coverage more budget-friendly. As Potter enjoys COVID-19 rage in the U.S., the former health care interactions executive stated Americans reside in "worry of having huge out-of-pocket costs without guarantee that we'll have our expenditures covered." With the number of uninsured Americans almost double what they were before novel coronavirus, according to some price quotes, Potter stated that is not sustainable.
reaction to the coronavirus pandemic was second-rate, if not the worst, in the world. This pandemic might bring the country to a snapping point, Potter said, pressing more Americans to require a health care system that goes beyond the reforms of the Affordable Care Act, which the Trump administration has actually consistently assaulted and tried to dismantle.
" You will see this project resurface to try to terrify people away from modification," he stated. "It takes place each time there is a significant push to change the health care system. The industry wishes to secure the status quo." There's no perfect healthcare system, and the Canadian system is not without flaws, Flood said.
In June 2019, New Democrat Celebration Leader Jagmeet Singh proposed broadening Canada's pharmaceutical drug coverage. The eventual objective of these modifications that have actually been debated in differing degrees for years is to encompass dental, vision, hearing, mental health and long-lasting care to produce "a head to toe healthcare system." And yet it is natural for Canadians to compare systems with their next-door neighbors and merely "feel grateful for what they have (how did the patient protection and affordable care act increase access to health insurance?)." She says that kind of complacency has insulated Canada's system from additional improvements that produce normally much better results for lower expenses, as in the UK, the Netherlands or Switzerland.
The 7-Second Trick For A Health Care Professional Is Caring For A Patient Who Is About To Begin Receiving Acyclovir
Health care reform has been an ongoing debate in the U.S. for decades. 2 terms that are often utilized in the discussion are universal healthcare protection and a single-payer system. They're not the exact same thing, regardless of the fact that individuals sometimes use them interchangeably. how does universal health care work. While single-payer systems normally consist of universal protection, lots of countries have attained universal coverage without using a single-payer system.

Universal protection refers to a healthcare system where every person has health coverage. According to the U.S. Census Bureau, there were 28.1 million Americans without health insurance in 2016, a sharp decline from the 46.6 million who had been uninsured prior to the execution of the Affordable Care Act (ACA).
Therefore, Canada has universal healthcare coverage, while the United States does not. It is necessary to note, nevertheless, that the 28.5 million uninsured in the U.S. includes a substantial variety of undocumented immigrants. Canada's government-run system does not provide protection to undocumented immigrants. On the other hand, asingle-payer system is one in which there is one entityusually the federal government accountable for paying health care claims.
So although it's a form of government-funded health coverage, the financing originates from 2 sources rather than one. People who are covered under employer-sponsored health insurance or private market health strategies in the U.S. (consisting of ACA-compliant plans) are not part of a single-payer system, and their medical insurance is not government-run.
There are currently at least 16 nations that use some form of a single-payer system, consisting of Canada, Norway, Japan, Spain, the UK, Portugal, Sweden, Brunei, and Iceland. In many cases, universal coverage and a single-payer system Visit this website go together, because a nation's federal government is the most likely candidate to administer and spend for a healthcare system covering countless people.
Fascination About A Health Care Professional Who Is Advising A Patient About The Use Of An Expectorant
Nevertheless, it is extremely possible to have universal protection without having a full single-payer system, and many countries around the globe have actually done so. Some countries run a in which the federal government offers basic healthcare with secondary protection offered for those can pay for a higher requirement of care. Denmark, France, Australia, Ireland, Hong Kong, Singapore, and Israel each have two-tier systems.

Interacted socially medication is another phrase that is often discussed in conversations about universal protection, however this design really takes the single-payer system one step further - how does universal health care work. In a socialized medication system, the federal government not only pays for healthcare but operates the medical facilities and utilizes the medical staff. In the United States, the Veterans Administration (VA) is an example of interacted socially medicine.
However in Canada, which also has a single-payer system with universal protection, the medical facilities are independently run and medical professionals are not used by the federal government. they merely bill the federal government for the services they offer. The main barrier to any socialized medicine system is the federal government's ability to successfully money, handle, and update its requirements, equipment, and practices to offer optimal healthcare.
